



An 11-year-old boy presents to the emergency department. While fishing, he was startled by a dog. He began to run away but tripped, landing on his rod. He immediately felt pain and noticed the fishhook had punctured his left index finger.
With summer comes outdoor activities — and ample opportunities for ED visits. Fishhook foreign body injuries generally present few complications and high satisfaction for patients and providers.1,2 Know these simple tricks for safe removal!
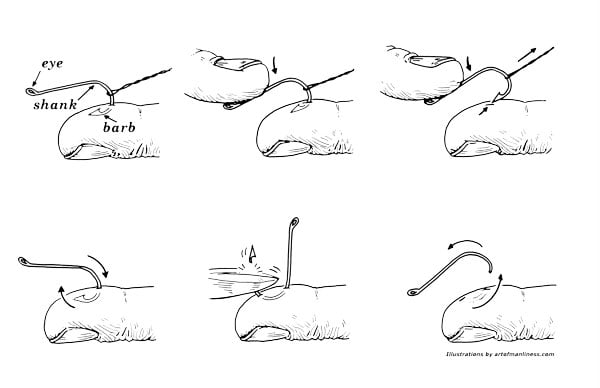 Top: String Yank Technique; Bottom: Advance and Cut Technique
Top: String Yank Technique; Bottom: Advance and Cut Technique Methods of Removal
Needle Cover
An 18- or 20-gauge needle can be used to remove superficial or treble hooks. After anesthetic is applied, the needle is inserted to cover the fishhook barb and thus disengage it from the embedded tissue. The needle and barb can then be simultaneously removed.3-5
String Yank Technique
The string yank technique is quick and anesthetic-free. Wrap a piece of 0-nylon around the hook to secure it. Exert downward pressure on the fishhook eye to disengage the barb. While holding the nylon, forcefully yank 180 degrees from the site of insertion. This method is often successful if an abrupt, forceful yank can be applied without hesitation.3-5
Advance and Cut
This technique is generally preferred.Using needle drivers, advance the hook to penetrate through the skin surface. Clip the barb with ring cutters or flatten it with pliers. Then, a smooth retrograde removal can be completed. This technique will require anesthetic and carries the most potential for tissue trauma.3-5
The Data
A prospective study of 97 cases of hook injuries noted 100% success rate when utilizing the above techniques.3 The advance and cut technique was the method of choice in 56/97 cases, while the needle cover and string yank were each chosen in 7/97 cases. Interestingly, 17/97 cases were removed only with a simple retrograde technique involving downward pressure and reversal along the hook's curvature.
Analgesia and Safety
Lidocaine may be required for patient comfort and safe removal of the hook. Digital blocks are effective in injuries only involving the digits. Given that the hooks may land unpredictably, it is important for the patient and the provider both to have proper eye protection.
Casting a Lifeline
In cases involving the eyelid or eye, prompt ophthalmology consult can help prevent vision loss or damage due to globe injury.1
In other unique cases involving bone or vascular penetration, consult orthopedists and vascular surgeons.4,5
Antibiotic and Immunization Prophylaxis
While no official guidelines exist, antibiotics are generally not indicated.4,5 However, consider antibiotics in special patient populations, including the immunocompromised and those with tendon, cartilage, or ocular involvement.1,4,5 In cases of cellulitis, antibiotic coverage should account for staphylococcus aureus and group A streptococcus bacteria. Consider antibiotics if there is concern for bacterial exposure common to bodies of water, such as Vibrio or Aeromonas.4,5 Any doubt regarding a patient's tetanus immunization status within the past 5 years warrants a tetanus booster because of the penetrating injury caused by the hook.
Case Resolution
The string yank method failed. An x-ray was obtained because of concern for bony involvement but only showed superficial penetration. A digital block was performed, and advance and cut method effectively removed the fishhook. Tetanus prophylaxis was given but no antibiotics were prescribed. Follow-up was recommended with his family physician.
References
- Aiello L, Iwamoto M, Guyer D. Penetrating ocular fishhook injuries: surgical management and long-term visual outcome. Ophthalmology. 1992;99(6): 862-866.
- Swanson JL, Augustine JA. Penetrating intracranial trauma from a fishhook. Ann Emerg Med. 1992;21(5):568-571.
- Doser C, Cooper WL, Ediger WM, et al. Fishhook injuries: a prospective evaluation. Am J Emerg Med. 1991;9(5):413-415.
- Gammons MG, Jackson E. Fishhook removal. Am Fam Physician. 2001;63(11):2231–2236.
- Stone DB, Scordino DJ. Foreign body removal. In: Roberts JR, ed. Roberts and Hedges' Clinical Procedures in Emergency Medicine. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014.