



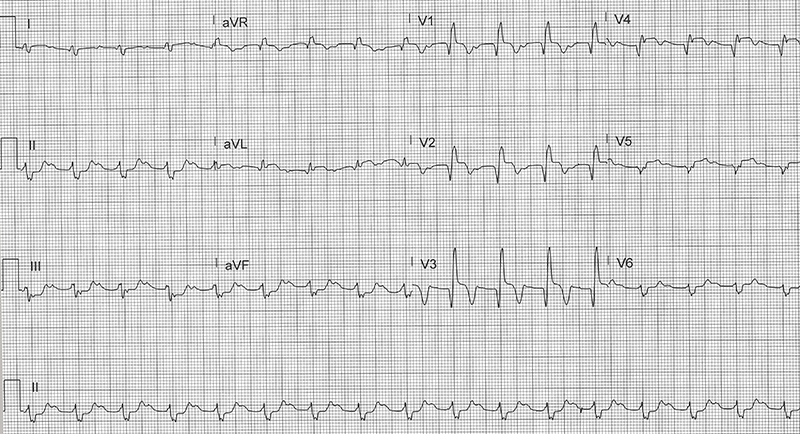
A 67-year-old male with a PMH of HTN, HLD, DM, and COPD presents to the emergency department due sudden chest discomfort. What is your interpretation of his ECG?
Answer
This ECG shows a normal sinus rhythm at 99 bpm, northwest/extreme axis deviation, 1st degree AV block, prolonged QRS complex duration with a RBBB, STE in leads II and V2-V5, and STD in leads II, III, and aVF. These findings are consistent with an anterolateral STEMI.
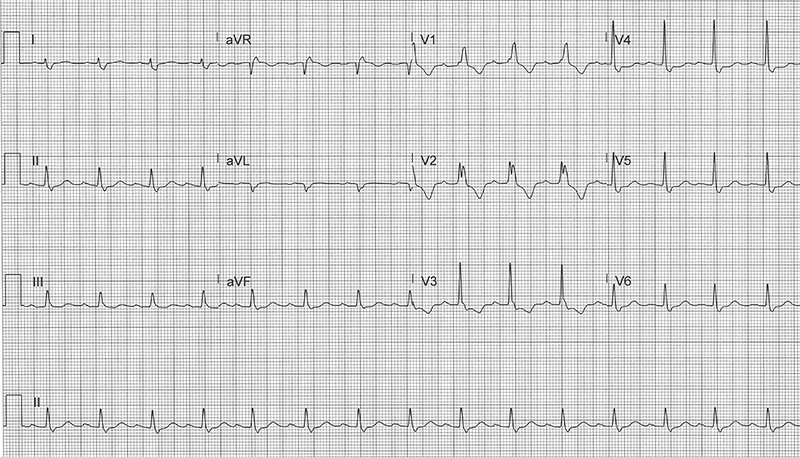
The characteristic findings in a normal RBBB (see Figure 1) include:
- QRS complex duration ≥ 120 msec
- rsr’, rsR’, or rSR’ pattern in lead V1 +/- V2
- Variation in lead V1 include qR pattern or broad R-wave that is often notched
- In lead V1, the initial upward deflection should always be smaller than the 2nd upward deflection
- S-wave duration > R-wave or > 40 msec in leads I and V6
- Normal R-wave peak time in leads V5 and V6 but > 50 msec in lead V1 (only required if broad R-wave +/- notch is present in lead V1)
- Expected repolarization abnormalities include STD and TWI in lead V1 +/- lead(s) V2-V3 if they have an rsR’ pattern, so STE and/or upright T-waves in those leads are concerning for ischemia
Figure 1. ECG showing a normal RBBB with expected repolarization abnormalities
In normal cardiac conduction, impulses travel equally down the left and right bundles in a near simultaneous manner. When there is a RBBB, the left ventricle is activated normally, but there is a delay in depolarization across the right ventricle which produces a secondary R-wave (R’) in the right precordial leads and a wide or slurred S-wave in lateral leads. In an isolated RBBB, left ventricular depolarization is unchanged so the axis is typically normal. A RBBB with an axis deviation should prompt evaluation for a concurrent left anterior or posterior fascicular block.
A RBBB will typically have STD and TWI in lead V1, and if leads V2-V3 have an rsR’ pattern present, they will also show this pattern. Consequently, upright T-waves or STE in those leads with an rsR’ pattern is concerning for ischemia, and even isoelectric or minimally elevated ST-segments can be a subtle indicator of early AMI. In this case, the presence of reciprocal STD in the inferior leads supports, but is not required for, the diagnosis of an MI.
In general, the presence of a RBBB does not confound the ECG evaluation of ACS as does a LBBB which requires the use of Sgarbossa criteria. Notably, patients presenting with a new RBBB in the setting of an anterior STEMI have a higher rate of acute heart failure, complete heart block, need for a permanent pacemaker, and a higher 30-day in-hospital mortality.1
Case Conclusion
This patient was taken to the cardiac catheterization laboratory where a 99% occlusion of the LAD was successfully treated with a stent. The patient was discharged home 3 days later in good health.
RBBB Learning Points
- Delayed conduction through right ventricle with normal left ventricular conduction
- In lead V1, the initial upward deflection should always be smaller than the 2nd upward deflection
- Repolarization abnormalities include STD and TWI in lead V1 +/- lead(s) V2-V3 if they have an rsR’ pattern, so STE and/or upright T-waves in those leads are concerning for ischemia
- Otherwise, the presence of a RBBB does not confound the ECG evaluation of ACS as does a LBBB
- RBBB with axis deviation should prompt evaluation for a concurrent LAFB or LPFB
Reference
- Shrivastav R, Perimbeti S, Casso-Dominguez A, Jneid H, Kwan T, Tamis-Holland JE. In Hospital Outcomes of Patients With Right Bundle Branch Block and Anterior Wall ST-Segment Elevation Myocardial Infarction (From a Nationwide Study Using the National Inpatient Sample). Am J Cardiol. 2021 Feb 1;140:20-24. doi: 10.1016/j.amjcard.2020.10.052. Epub 2020 Nov 2. PMID: 33147431.