



A 65-year-old female with history of thoracic aortic aneurysm s/p aortic graft repair several years ago presented to the ED with positive blood cultures on outpatient labs. These had been ordered by her PCP secondary to 2 weeks of fevers and malaise. Other history is notable for a dental extraction 3 weeks ago. What is your interpretation of her ECG?
Answer
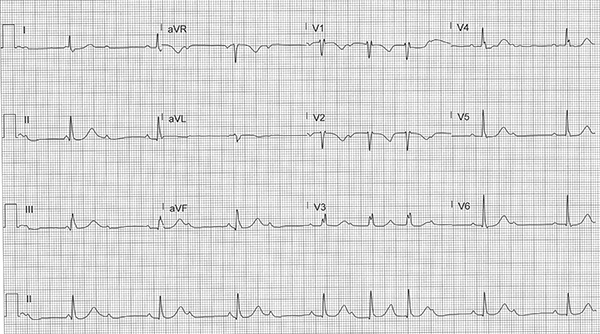
This ECG show an irregular narrow-complex bradycardia with an average ventricular rate of 48 bpm, a regular atrial rate of 86 bpm, normal axis, variable PR intervals, and normal QTc interval.
The differential diagnosis for an irregular narrow complex rhythm with bradycardic ventricular rates includes:
- Atrial fibrillation (rate controlled)
- Atrial flutter with variable block (rate controlled)
- Atrial tachycardia with variable block (rate controlled)
- Wandering atrial pacemaker
- 2nd degree AV block Mobitz types I and II
- Variable high-grade AV block (eg, 3:1, 4:1, etc.)
- 2nd degree sinoatrial block
- Sinus arrhythmia
- Sinus bradycardia, junctional rhythm, or junctional bradycardia with irregular pattern of PAC, PJC, and/or PVC
- Sinus bradycardia, junctional rhythm, or junctional bradycardia with regular patterns of PAC, PJC, and/or PVC (bigeminy, trigeminy, etc.)
The key to interpreting this ECG is recognizing that the P-waves march out (ie, there is a regular PP interval, see Figure 1). This narrows the differential to a 2nd degree AV block and/or variable high-grade AV block. Note that atrial tachycardia with variable block will show regular P-waves with an irregular ventricular rhythm but requires an atrial rate of 150-250 bpm, which is not seen in this ECG.

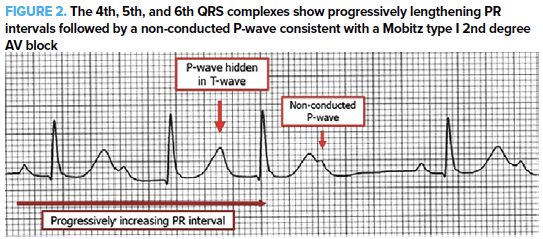
This ECG is a hodgepodge of AV blocks. The 1st QRS complex is likely a junctional escape beat as the preceding PR interval is too short for there to be normal sinus conduction. This is followed by a 2nd degree AV block with 2:1 AV conduction for 2 beats. The 4th, 5th, and 6th QRS complexes have progressively lengthening PR intervals followed by a non-conducted P-wave (see Figure 2), consistent with a Mobitz type I 2nd degree AV block. The penultimate beat shows a 2nd degree AV block with 2:1 AV conduction. There is a P-wave that is partially hidden in the T-wave of the last beat, but the ECG cuts off before the type of block can be determined (eg, 2-1 AV conduction, Mobitz type I, etc.).
Case Conclusion
This patient remained in 3rd degree AV block and became hypotensive, requiring transvenous pacing in the ED. She was admitted to the ICU, and blood cultures came back positive for Streptococcus mitis, a viridans group Streptococcus species commonly associated with endocarditis from a dental source (the bacteria was named for the mitral valve, off of which it was first isolated). A subsequent transesophageal echocardiogram was within normal limits, making endocarditis extremely unlikely. A cardiac PET scan was obtained due to her history of ascending aortic aneurysm repair and confirmed the diagnosis of aortic graft infection. Although infrequent, aortic graft infections can lead to 2nd or 3rd degree AV blocks due to the proximity of the AV node and bundle of His to the aortic valve and root.
2nd degree AV Block with 2:1 Conduction Learning Points
- 2nd degree AV block with 2:1 conduction will show blocked conduction of every other P-wave
- It is not always possible to determine if the underlying block is a Mobitz type I or type II, so assume the higher risk Mobitz type II conduction
Mobitz type I AV Block Learning Points
- Progressively increasing PR interval and decreasing RR interval until a non-conducted P-wave occurs (i.e., P-wave without accompanying QRS complex)
- PR interval immediately after non-conducted P-wave is shorter than PR interval preceding non-conducted P-wave
- RR interval that includes non-conducted P-wave < twice the PP interval
- Can be normal variant and usually does not produce hemodynamic compromise
- Typically associated with excess vagal tone and therefore usually responds to atropine when acute treatment is needed
- Can lead to a more advanced AV block if associated with a pathologic etiology
- Can be seen with inferior MI