



Case:
A 56-year-old female with a history of chronic kidney disease and hypertension presents with diffuse weakness and fatigue over the past 3 days.
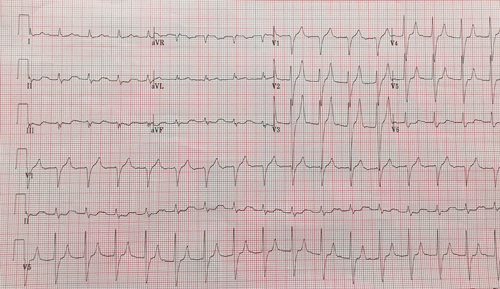
What are you seeing in this ECG?
ANSWER
This ECG demonstrates an accelerated idioventricular rhythm (AIVR) with peaked T-waves in the septal leads. Given the patient’s renal disease, hyperkalemia should be considered.
A systematic approach to reading ECGs will help prevent overlooking important subtleties. The rate is about 100 with a regular, wide-complex rhythm. There are no p waves. Regular, wide complex tachycardia without p waves should always prompt a consideration of ventricular tachycardia (VT). However, true VT tends to have a rate closer to 120 beats per minute (bpm). A lack of p waves in the presence of a regular rhythm suggests that the heart’s pacing is originating from a focus below the atria. This includes the AV node (“junctional rhythm”) or the ventricles.
In the setting of a wide QRS complex, this must be either an idioventricular rhythm or a junctional rhythm with an associated bundle branch block (BBB). To understand this, we must first recall that the QRS segment represents ventricular depolarization. In a normal heart, this conduction pathway proceeds through the typical Bundle of His → bundle branches → purkinje fiber pathway. Any changes to this will create a widened QRS. These are generally secondary to BBBs, accessory pathways, or rhythms originating from the ventricles, called idioventricular rhythms. Therefore, this patient has either an accelerated junctional rhythm with LBBB or AIVR. Ultimately, this patient was found to be profoundly hyperkalemic. Her ECG normalized with treatment of her hyperkalemia.
Learning Points
- The differential for regular, wide complex tachycardias include ventricular tachycardia, supraventricular or junctional rhythms with bundle branch blocks, or an idioventricular rhythm.
- Causes of AIVR include electrolyte abnormalities, ischemia/infarction, structural disease, and medications (ie, digoxin toxicity).
- Treatment of AIVR includes ensuring patient stability, and identifying and treating the underlying cause.
- Hyperkalemia may mimic many other conduction abnormalities.