



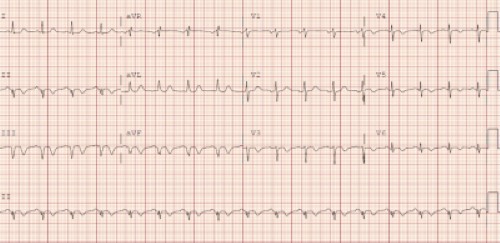
A 62-year-old male presents with chest pain that has been gradually worsening over the past 2 weeks. What is your interpretation of his ECG?
Answer
This ECG shows sinus tachycardia at 102 bpm, left axis deviation, normal intervals, TWI in leads II, III, aVF, and V3-V6, and Q-wave in leads II, III, and aVF.
Q-waves are the initial negative deflection that precede the upright R-wave of the QRS complex and can be pathological or non-pathological. Pathologic Q-waves are generally defined as ≥40 msec and/or ≥ 25-33% of accompanying R-wave height. Causes of pathologic Q-waves include structural, conduction, and/or myocardial etiologies (see table below in Learning Points).
A QS complex is used to describe a single large negative deflection, which is seen in leads III and aVF in the case ECG. When associated with ischemia, QS complexes typically indicate significant irreversible myocardial loss. When associated with recent MI, QS complexes with STE and diminished T-waves, typically seen in the precordial leads, should prompt evaluation for LV aneurysm.
In the past, MIs were classified as Q-wave MI and non-Q-wave MI. These terms are no longer used, but misconceptions based on this classification system persist. Current cardiology research has shown:
- Q-waves do not predict viability of myocardium
- Q-waves correlate with size of the infarction but do not differentiate between transmural and non-transmural/subendocardial infarction
- Large Q-waves that suggest a large infarction are associated with a high risk for LV dysfunction, but LV dysfunction can occur in the absence of Q-waves
- Q-waves associated with infarction are not permanent and can resolve or diminish over time
Case Conclusion
Cardiology was emergently consulted and took the patient to the cardiac catheterization lab, where a proximal RCA occlusion was successfully stented.
Q-waves Learning Points
- Can be pathological or non-pathological
- Pathologic Q-waves generally defined as ≥40 msec and/or ≥ 25-33% of accompanying R-wave height
- When due to an MI:
- Occur in ≥ 2 contiguous leads that also have STE
- Size correlates with volume of infarcted myocardium
- Early appearance of Q-waves does not always indicate irreversible myocardial death, particularly with simultaneous STE and/or shorter period of ACS symptoms
- Tall R-waves in leads V1 and V2 may represent Q-waves due to a posterior MI
- QS complex = single large negative deflection
- Usually indicates significant irreversible myocardial loss when associated with ischemia
- QS complex with STE and diminished T-wave should prompt evaluation for LV aneurysm
- Q-waves in leads V1 and V2 can be caused by misplacement of leads in the 2nd or 3rd intercostal spaces
|
Causes of Pathologic Q-waves |
|
|
Structural |
LVH RVH HCM |
|
Conduction |
LBBB Pre-excitation rhythms |
|
Myocardial |
Infarction Cardiomyopathy Myocarditis Infiltrative disease |