



A 36-year-old female with a PMH of alcohol use disorder and type 1 DM presents with substernal chest tightness, nausea, vomiting, and diaphoresis. What is your interpretation of her ECG?
Answer
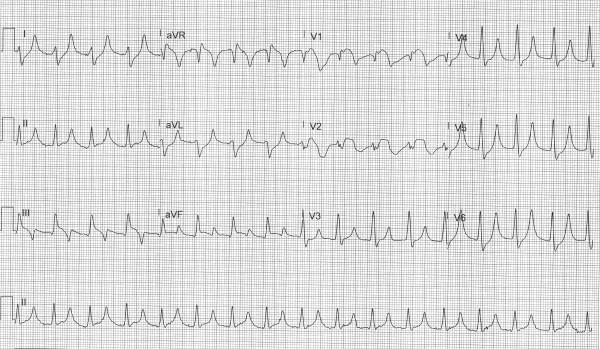
This ECG shows a regular wide complex rhythm with a ventricular rate of 100 bpm, no discernable P-waves, right axis deviation, and a prolonged QRS complex duration of 160 msec with an intraventricular conduction delay. There are large T-waves in leads I, II, aVL, aVR, and V4-V6, STE in leads III, aVF, aVR, and V1-V2, and STD in leads I, aVL and V4-V6.
This EKG could easily be interpreted as a STEMI, especially given the patient’s symptoms, but the constellation of findings suggests hyperkalemia which can cause STE, especially in leads V1-V2, that mimic a STEMI.1 This patient was aggressively treated with IV calcium gluconate (8 amps in the first 20 minutes), insulin with dextrose, and IVF. Nebulized albuterol was deferred due to COVID and a lack of available negative pressure rooms. Figures 1-3 demonstrate the dynamic ECG changes seen over the first hour of treatment.
Figure 1. Repeat ECG 15 minutes later
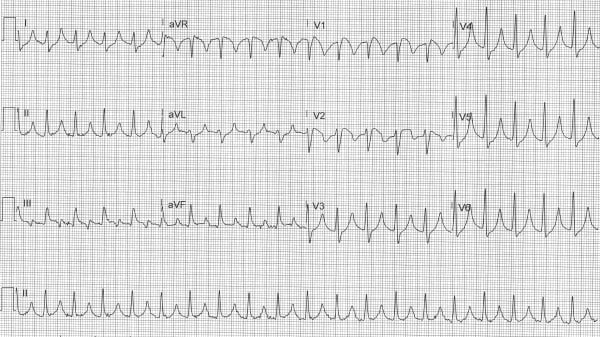
Figure 2. Repeat ECG 30 minutes later
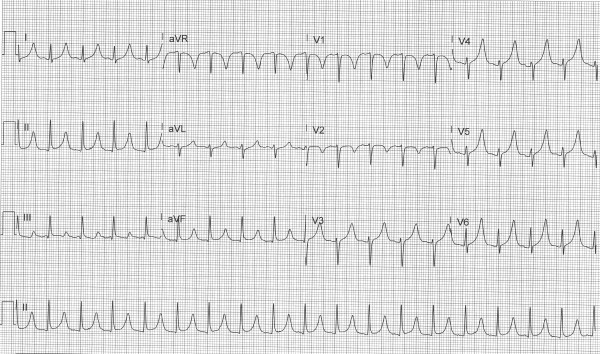
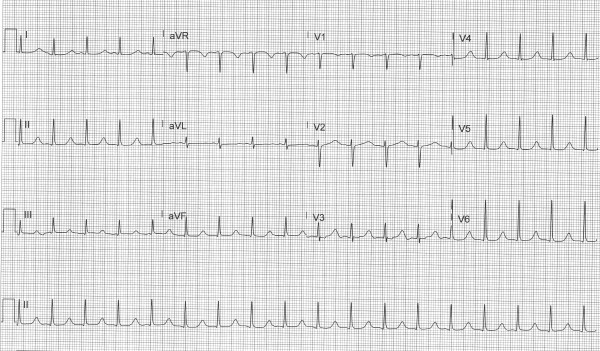
Figure 3. Repeat ECG 60 minutes later
Case Conclusion
This patient’s initial labs showed multiple abnormalities consistent with severe DKA, as well as a potassium level of 7.8 mEq/L. She was admitted to the ICU for further treatment.
Regarding the dose of calcium used in this case, there are no universally accepted guidelines for the dosing of calcium in the treatment of hyperkalemia. In cases of severe hyperkalemia, it is reasonable to treat aggressively with calcium as the risk of inadequately treated hyperkalemia outweighs the risk of iatrogenic hypercalcemia.
Hyperkalemia Learning Points
- ECG is specific but not sensitive for hyperkalemia (ie, hyperkalemia can present with minimal to no ECG changes)2
- ECG changes are not always sequential/progressive and include:
- Tall, narrow, peaked T-waves (best seen in the precordial leads)
- P-wave flattening and PR interval prolongation
- Prolonged QRS complex duration, ranging from minimal to maximal
- Conduction abnormalities (AV blocks, fascicular and bundle branch blocks)
- Bradycardia
- Sino-ventricular rhythm (loss of P-waves, extremely widened QRS) with normal or slow rate
- Ventricular dysrhythmias
- Hyperkalemia can mimic a broad range of pathologies
- Can cause STE (common in leads V1-V2 and aVR) that mimics a STEMI or Brugada pattern
- Can also occur simultaneously with hyperacute T-waves and obscure early changes seen in an anterior or anteroseptal AMI
References
- Dendramis G, Massimo Petrina S, Baranchuk A. Not all ST-segment elevations are myocardial infarction: Hyperkalemia and Brugada phenocopy. Am J Emerg Med. 2017;35(4): 662.e1-662.e2.
- Rafique Z, Kosiborod M, Clark CL, et al. 61 Electrocardiogram Changes Are Not Reliably Associated with Hyperkalemia or Its Severity. Ann Emerg Med. 2017;70(4): S25-S26.