


Case
A healthy 29-year-old male presented to the ED complaining of right forearm pain and swelling after a strangulation-type injury that occurred 5 hours prior to arrival. While water skiing, there was a miscommunication between him and the operator of his boat, leading to the boat accelerating at full speed while a rope was wrapped around his forearm. The patient was yanked forward but was able to untangle his arm after approximately 20 seconds. He immediately presented to an outside ED, where a forearm x-ray performed showed no fracture. However, during his stay at that hospital he required numerous doses of narcotic pain medication to achieve analgesia. He was subsequently discharged home with ibuprofen.
As seen in community ED:

After worsening pain, the patient presented to a tertiary care facility near his home. He was subsequently admitted to the orthopedic surgery service for observation and pain control, with plans to discharge in the morning if he felt better. Unfortunately for the patient, he awoke the next morning with worsening pain, swelling, and decreased function of his right hand. The decision was made to take him emergently to the OR, and extensive forearm fasciotomies were performed. Intraoperatively, he was found to have significant hematoma and injury throughout the volar compartment, leading to compartment syndrome. The patient tolerated the procedure well and was discharged home the next day.
One week post-op:

Discussion
Orthopedic complaints account for a significant percentage of emergency department visits annually throughout the United States. The majority of these patients do not have life or limb threatening injuries and are often triaged as low acuity. Compartment syndrome, on the other hand, is a true orthopedic emergency and providers must have a high index of suspicion to detect this limb-threatening pathology.
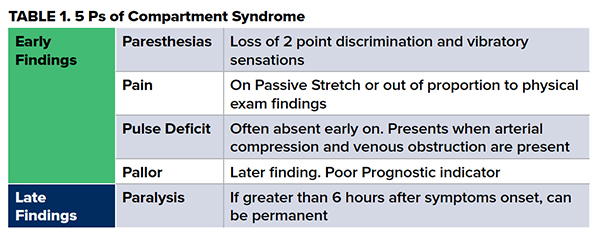
Compartment syndrome occurs when elevated pressure within the muscular compartment of a limb prevents venous drainage. This, in turn, disrupts arterial perfusion to the muscles and nerves within that compartment. If not detected in a timely fashion, compartment syndrome can lead to ischemia, infarction, and Volkmann’s contractures. While it is typically seen in the setting of fracture, it can occur in any situation where there is increased content, decreased volume, or prolonged external pressure in or on a compartment. Other, less commonly seen, causes of compartment syndrome include prolonged downtime in a fixed position, intensive use of a muscle during exercise or seizure, excessive traction on a fractured limb, leaking dialysis cannula, or pressure infusions. Classically, the symptoms of elevated compartment pressure are taught as the “5 Ps" (Table 1). However, delaying diagnosis until all findings are observed can be a critical mistake.
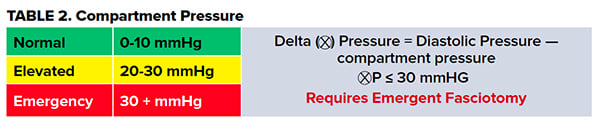
While compartment syndrome is a clinical diagnosis, measuring compartment pressures can assist in its diagnosis. Pressure measurements are obtained via manometry, commonly by using a Stryker tonometer. Normal compartment pressure is 0-10 mmHg. Emergent fasciotomy should be considered at pressures greater than or equal to 30 mmHg. The delta pressure can also be obtained as a surrogate marker of compartment perfusion (Table 2).
Once the diagnosis of compartment syndrome has been established, either clinically or by tonometry, immediate intervention must take place. The gold standard for treatment of compartment syndrome is fasciotomy. This procedure should be performed by a surgeon, but can be performed by emergency medicine physicians if in an austere or isolated practice environment. Patients who have elevated pressures or symptoms concerning for development of compartment syndrome with an appropriate mechanism deserve admission to the hospital for observation and serial examinations.
Conclusion
There are very few orthopedic emergencies, but compartment syndrome is without a doubt one of them. Timely diagnosis and definitive management are essential in preventing limb threatening injury and long term complications. When in doubt, call your friendly orthopedic surgeon for assistance.
References
1. Roberts JR, Custalow CB, Hedges JR, Thomsen TW. Roberts and Hedges Clinical Procedures in Emergency Medicine. Philadelphia: Elsevier/Saunders; 2014.
2. Marx JA, Hockberger RS, Walls RM. Rosen’s Emergency Medicine: Concepts and Clinical Practice. Philadelphia: Elsevier/Saunders; 2014.
3. Adams JG. Emergency Medicine: Clinical Essentials. Philadelphia: Elsevier Saunders; 2013.
4. Lee B, Riddell J. Orthopedic Emergencies: When to Ask for a Little Help from Our Friends. emDOCs.net - Emergency Medicine Education. http://www.emdocs.net/orthopedic-emergencies-when-to-ask-for-a-little-help-from-our-friends/. Published April 9, 2018. Accessed July 21, 2019.
5. Wiesel SW, Delahay JN, Sankar, WN, Wiesel BB. Orthopaedic Surgery: Principles of Diagnosis and Treatment. Philadelphia: Wolters Kluwer, Lippincott Williams & Wilkins; 2011.
6. Via AG, Oliva F, Spoliti M, Maffulli N. Acute compartment syndrome. Muscles Ligaments Tendons J. 2015;5(1):18-22.