



In 2018, statistics show 15,605 children and adolescents were confirmed victims of physical abuse in the United States. It is vital to ensure a safe disposition for pediatric patients, as further harm is compounded if child maltreatment goes unrecognized.
Emergency physicians are responsible for making the first clinical decisions when treating patients; however, the natural history of a disease in a patient that presents for care is not always witnessed. In cases of suspected child maltreatment, the initial evaluation in the emergency department may not be conclusive in assessing for occult injuries in an infant that presents for care by the time of discharge. However, it is vital to ensure a safe disposition for the child as further harm is compounded if child maltreatment goes unrecognized. The following case and discussion emphasize the significance of a follow up skeletal survey (FUSS) in cases of suspected non-accidental trauma (NAT).
Data from the United States Department of Health and Human Services’ Child Maltreatment Report found that in 2018, 15,605 children and adolescents were confirmed victims of physical abuse in the United States. The data showed that 84.5% of victims suffered a single type of maltreatment, with 60.8% of these patients neglected, 10.7% physically abused, and 7% sexually abused; 15.5% of patients were victims of 2 or more maltreatment types. Children under the age of 1 year are the most vulnerable to maltreatment and comprise 26.7% of total victims1 and approximately 23% of the child maltreatment fatalities.
With all cases of suspected non-accidental trauma, emergency physicians should initiate a work-up to assess for other injuries. In young children, this evaluation often includes a detailed history and a physical examination, radiographs, and laboratory testing including a CBC with differential, AST, ALT, lipase level, and a urinalysis.2 Depending on the type of injuries observed (ie, bruising, fractures, intracranial injury), further testing may be indicated. In cases of bruising, a hematological work up (PT/PTT/INR, Fibrinogen, vWF Ag, VWF activity, Factors 8 and 9) should be considered to rule out any bleeding disorders confounding exam findings. Head imaging should be obtained in the event the child is less than six months old, or there is evidence of head/facial trauma, or if the patient has an abnormal neurologic exam. An abdominal CT may be indicated if laboratory values or physical exam are concerning for occult hepatic or pancreatic injury.2 Finally, in non-skull fractures, calcium, phosphorus, Vit D, intact PTH, and alkaline phosphatase levels should be obtained. A skeletal survey (SS) should be obtained in all children less than 2 years of age with a suspicious injury. The use of skeletal surveys in children 2-5 years of age varies widely, with some cases reporting 36-45% of these patients receive a skeletal survey in the case of suspected non-accidental trauma.3 This is likely due to the fact that most sources recommend that the decision about obtaining a SS in the 2- to 5-year-old age group must be made individually on the basis of the specific clinical indicators of abuse, such as bruises in the TEN 4 FACES region, as well as any high specificity fractures, such as classic metaphyseal lesions (CMLs), rib fractures (especially posteromedial), scapular fractures, spinous process fractures, and sternal fractures.5-7 Multiple fractures, fractures of different ages, and complex skull fractures are of moderate specificity for NAT, but again may necessitate the need for a skeletal survey on a case-by-case basis.7
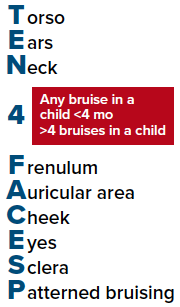
Figure 1. Body region- and age-based bruising clinical decision rule to identify children who are at high risk for abuse and require further evaluation4
During the course of evaluating for NAT, a skeletal survey may reveal occult injuries such as rib fractures or CMLs. These fracture types have a high specificity for abusive injury in infants; however, acutely, they may not be radiographically apparent. The AAP recommends follow up skeletal surveys 2-3 weeks after the initial survey, as these fracture types are more radiographically apparent once they start to heal. Multiple studies have documented the utility of follow up skeletal surveys. In one study, secondary data from the ExSTRA (Examination of Siblings To Recognize Abuse) Study evaluated the rates of FUSS in suspected NAT and the yield of new information. 2049 children were included in the study who had an initial SS. 38.8% of these children underwent a FUSS. A total of 174 (21.5%) subjects had new information identified by FUSS, including 124 (15.6%) with at least 1 new fracture; resulting in an increased estimated likelihood of abuse in 41 (33%) cases. Of those with new fractures found on FUSS, the most common were of the ribs, long bones and metaphyseal lesions. In addition, an initial negative SS followed by a positive FUSS occurred in 7.1% (n = 18) of cases.8
Case Discussion
A 3-week-old boy presented to the ED for increased fussiness. Mother stated that the patient had been increasingly fussy over the past 2 nights and became inconsolable. On the morning of presentation, she noticed a new "rash" on his right upper arm. His mother reported she was the primary caretaker with help from a family member who last helped 2 days prior, and the morning of arrival. The patient was born via vaginal delivery at 36 weeks gestational age due induction of labor for maternal preeclampsia, otherwise without complication. He received Vitamin K at birth. The remainder of history and review of symptoms were normal.
The physical examination revealed well demarcated, linear, non-blanching red-purple lesions on anterior surface of the right forearm, consistent with bruising. Similar lesions were found on the posterior right shoulder, the back, and scattered areas on the right upper arm. The remainder of the physical exam was normal for age.

Image 1. Linear non blanching red-purple lesions, consistent with bruising
Because of the presence of unexplained bruising in this 3-week-old, a NAT work-up was initiated. CT scan of the head, skeletal survey, and screening trauma labs (CBC, AST, ALT, Lipase, UA) were obtained. Because of the presence of bruising, additional hematological studies (PT/PTT/INR, Fibrinogen, vWF Ag, VWF activity, Factors 8 and 9) were also ordered. The patient was subsequently admitted for further evaluation and a report was filed with the local child protective services (CPS) agency, with consultation by the hospital's child abuse team.
The patient's head CT and all laboratory studies resulted as normal. The initial skeletal survey did not show any radiographic evidence of injury. A follow-up skeletal survey was recommended by the child abuse team.
A safe plan of discharge was identified for the patient by CPS while their investigation was in place with child abuse team follow-up.
A FUSS was completed 2 weeks later.
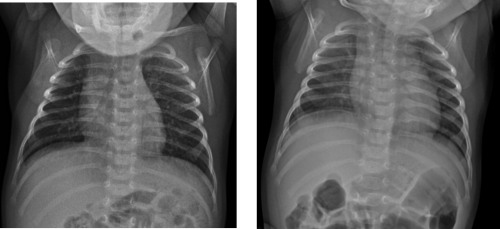
Image 2. AP chest radiograph. A. Normal. B. Follow up, demonstrates healing changes with callus formation from the left second through eighth costovertebral junction
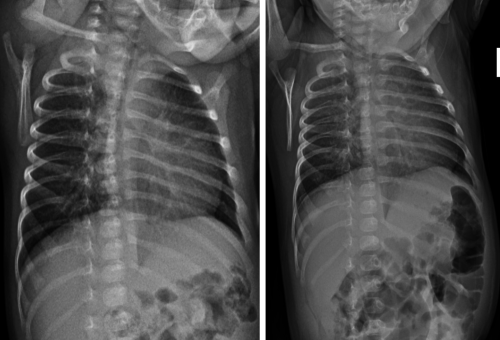
Image 3. Oblique views of left ribs. AP chest radiograph. A. Normal. B. Follow up, demonstrates healing changes with callus formation from the left 2nd through 8th costovertebral junction
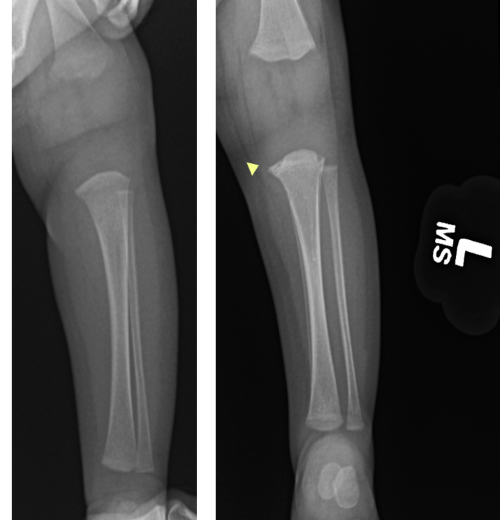
Image 4. Frontal view of left tibia and fibula. A. Normal. B. Follow up. Irregularity of proximal tibial metaphysis, concern for healing classic metaphyseal lesion
Take-Home Points
- When considering similar cases, with fractures seen on the second skeletal survey, it is clear why the FUSS is so important and should be at the forefront of the clinician’s mind when making disposition recommendations for a patient who has undergone non-accidental trauma evaluation.
- It is critically important to realize that child maltreatment may often have a normal exam and workup with no physical, radiographic, or laboratory abnormalities.
- Close follow-up with a child abuse pediatrician and a second skeletal survey are vital to ensure completion of the initial child abuse evaluation and ultimately the well-being and safety of the child.
References
- US Department of Health and Human Services, Administration on Children, Youth, and Families. Child Maltreatment 2018. Washington, DC: US Government Printing Office.
- The Evaluation of Suspected Child Physical Abuse. Cindy W. Christian, Committee on Child Abuse and Negect. Pediatrics. 2015;135(5):e1337-e1354.
- Wood JN, Fakeye O, Feudtner C, Mondestin V, Localio R, Rubin DM. Development of guidelines for skeletal survey in young children with fractures. Pediatrics. 2014;134(1):45–53.
- Pierce MC, Kaczor K, Aldridge S, O'Flynn J, Lorenz DJ. Bruising Characteristics Discriminating Physical Child Abuse From Accidental Trauma. Pediatrics. 2010;125(1):67-74.
- Kleinman PK, Marks SC, Blackbourne B. The metaphyseal lesion in abused infants: a radiologic-histopathologic study. AJR Am J Roentgenol. 1986;146 (5):895– 905.
- Flaherty E, et al. Evaluating Children With Fractures for Child Physical Abuse. Pediatrics. 2014;133(2):e477-e489.
- Section on Radiology, American Academy of Pediatrics. Diagnostic imaging of child abuse. [policy statement] Pediatrics. 2009;123(5):1430–1435.
- Harper NS, Eddleman S, Lindberg DM, for the ExSTRA Investigators. The Utility of Follow-up Skeletal Surveys in Child Abuse. Pediatrics. 2013;131(3):e672-e678.