



We present a case of bradycardia and dyspnea in an otherwise healthy young male found to have EKG abnormalities inclusive of third-degree heart block.
He was determined to have secondary Lyme disease as his presenting clinical diagnosis and was admitted to the CCU and discharged later with a normal and resolved EKG with normal vital signs.
Case
A 29-year-old male with a history of childhood asthma presents for 7 days of dyspnea on exertion that is worsened with activity and improved with rest. He went to urgent care earlier and was told to go to the ED for an abnormal EKG. He is an avid cyclist and became worried when his activity was becoming limited. He denies any paroxysmal nocturnal dyspnea, orthopnea, lower extremity edema, any pulmonary embolism risk factors, history of deep venous thrombosis/pulmonary embolism, family history of arrhythmias, coronary artery disease, congestive heart failure, or myocardial infarction.
Additionally, he became worried when 3 days prior, his Apple watch told him his heart rate was between 30-39 bpm. He endorses a sharp pain in the epigastric/midsternal area when he has shortness of breath. He is also endorsing a fever (103 t max) today, and before this had a fever for 3 days with chills, myalgias, arthralgias, and intermittent dizziness when standing up too quickly. He had no sick contacts, cough, rhinorrhea, sore throat, and he tested negative for flu and covid twice. His EKG was obtained and was noted to be abnormal with 3rd degree heart block (Figure 1). Of note, he traveled to upstate NY for a hiking trip 1 month ago.
Figure 1. Initial EKG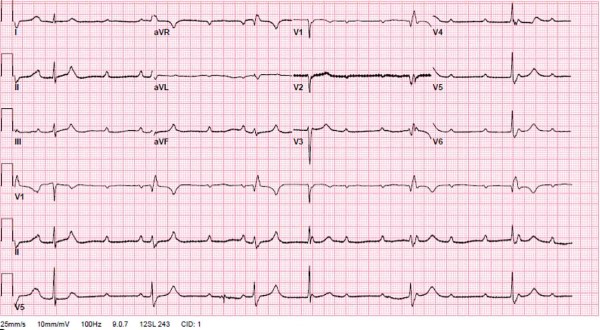
Additionally, he notes upon further questioning that 1 month ago, he had a bump on his left arm that was slightly itchy, which he thought was a mosquito bite and subsided with no further rashes. This rash appeared as a small circle. In the ED, the patient was noted to have stable vital signs originally, but then progressed to becoming bradycardic to 33, at which point he was brought to the resuscitation bay.
Diagnosis
Acute disseminated Lyme is an uncommon initial presentation of Lyme disease, especially with the initial rhythm showing a third-degree heart block on EKG We present a case in which the diagnosis was presumed to be disseminated Lyme disease complicated by third degree heart block based on clinical presentation, history, EKG, and Lyme serology. His Lyme serology were all positive, with a negative troponin, BNP, and lactate. He also had a normal white blood cell count; however, he did have increased inflammatory markers. He was then admitted to the CCU for further monitoring, intravenous antibiotics including ceftriaxone, and was discharged 3 days later with a totally normal EKG (Figure 2), resolution of symptoms, decrease in inflammatory markers, cardiology follow-up outpatient, and oral antibiotics.
Figure 2. Repeat EKG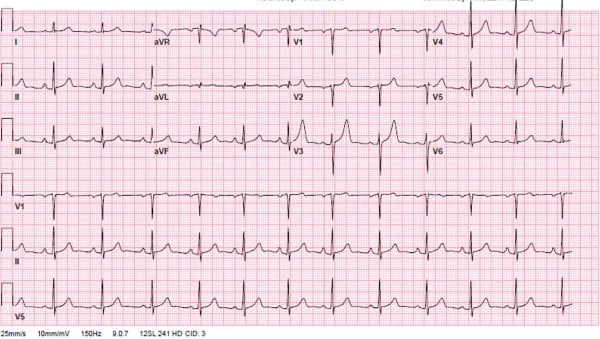
Lyme disease is the most common tick-borne disease in the U.S. and is caused by Borrelia burgdorferi. It is commonly spread by the ixodes tick, which also causes Anaplasmosis and Babesiosis. It is most frequently seen in the upper Midwest, Northeast, and mid-Atlantic states. Lyme has 3 stages, which include early, disseminated, and late.2
- Early phase occurs days to months after the bite and includes symptoms such as myalgias, arthralgias, fatigue, as well as the classic erythema migrans rash.
- Acute disseminated phase occurs weeks to months after the bite, (which is how our patient presented) and includes further dermatologic symptoms, neurologic manifestations such as cranial neuropathy (Bell’s palsy), radiculopathy, encephalopathy, and cardiac manifestations such as AV block, with third-degree block being the most common2. The pathophysiology of the AV block is not well understood; however, it is believed to be due to transmural inflammation caused to the myocardium.
- Late stage includes arthritis, commonly in the knee, and more severe neurologic manifestations such as psychiatric disturbance, encephalopathy, and memory impairment3.
There is a good prognosis in the early and acute disseminated stages with treatment, with resolution between 4-42 days.
Patients with cardiac manifestations and associated heart block frequently do not require cardiac pacing, and the third-degree block typically improves within a week. The drug of choice for this phase is ceftriaxone 2g IV, continuing until the AV block resolves and the PR is less than 300, at which point treatment is switched to a 14-21 day course of oral doxycycline or amoxicillin.1
Take-home Points
- Overall, our case highlights the importance of considering Lyme disease as an etiology of acute bradycardia with heart block in patients with shortness of breath or chest pain, in all ages, in endemic areas.
- It also demonstrates the rarity of this initial presenting diagnosis in an otherwise young and healthy patient with abnormal vital signs.
- Lastly, it discusses the importance of recognizing this diagnosis early through a thorough travel history and physical exam to initiate early intervention and prevent unnecessary cardiac pacemaking.
References
- Steere AC, Batsford WP, Weinberg M, et al. Lyme carditis: cardiac abnormalities of Lyme disease. Ann Intern Med. 1980;93(1):8-16.
- Forrester JD, Mead P. Third-Degree Heart Block Associated With Lyme Carditis: Review of Published Cases. Clin Infect Dis. 2014;59(7):996–1000.
- Riaz S, Garel A, Subedi A, Mogadam E, Weinberg A. Third-Degree Atrioventricular Block as the Initial Presentation of Lyme Disease. Cureus. 2020;12(8):e9574.
fix all citations