



Acetaminophen toxicity is one of the most common causes of liver toxicity in the United States.
Acetaminophen ingestions are the most common cases called into poison centers in the United States, accounting for more than 100,000 calls per year.1 Each year in the United States, acetaminophen overdoses are estimated to result in 56,000 emergency department visits, 2,600 hospital admissions, and 500 deaths.2 According to the United States Acute Liver Failure Study Group registry, 42% of all cases of acute liver failure in the United States are attributable to acetaminophen overdose.3
The therapeutic antipyretic mechanism of action is not well understood. However, acetaminophen is thought to inhibit COX receptors in the CNS selectively. Toxicity develops at 150 mg/kg or >7.5 g/day. Acetaminophen is metabolized by glucuronidation primarily to nontoxic metabolites. However, in large overdoses these pathways become saturated, and more acetaminophen is converted by CYP2E1 into the toxic metabolite N-acetyl-p-benzoquinone imine (NAPQI). As shifts toward the CYP2E1 pathway occur, glutathione serves to reduce NAPQI to nontoxic metabolites. Please reference image one. Glutathione stores become depleted in large acetaminophen overdoses and are subsequently unable to reduce all the generated NAPQI to its nontoxic metabolites. Glutathione depletion leads to more NAPQI and resultant hepatic necrosis. N-acetylcysteine (NAC) is the only Food and Drug Administration (FDA) approved antidote in acetaminophen toxicity and is the mainstay treatment for significant acute overdose. However, new data reveals that fomepizole may be hepatoprotective in high dose acetaminophen toxicity when reviewed in animal models, and possibly an effective adjunct to treatment regimens, especially in massive overdose or in unknown time of ingestion (TOI).4,5
Background/History
Conventionally used in methanol/ethylene glycol overdose, fomepizole acts to competitively inhibit alcohol dehydrogenase (Figure 1). This action reduces the formation of the toxic metabolites from the metabolism of methanol and ethylene glycol. Fomepizole also acts as a potent inhibitor of the CYP2E1 protein which is induced by acetaminophen.6 CYP2E1 is the primary driver for NAPQI formation, and this pathway would thus be inhibited by fomepizole administration. When used alongside NAC, which enhances the creation of glutathione, fomepizole can serve as an adjunct by inhibiting the conversion of acetaminophen to NAPQI.7,8 Although NAC has excellent data showing its efficacy in reversing detrimental acetaminophen effects when administered in the first 8-10 hours after ingestion, patient presentations are not always cut and dry.4,9 There are many reports of massive acetaminophen ingestions as well as delayed patient presentations in which NAC alone is unable to prevent or halt ongoing hepatic necrosis.4
Figure 1. The metabolism of acetaminophen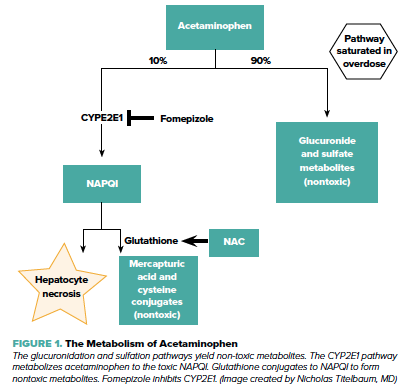
Dosing: When used for toxic alcohols, the dose of fomepizole is 15 mg/kg IV over 30 min; followed by 10 mg/kg q12hrs for 4 doses until the toxic alcohol level is < 20 mg/dL or acidosis resolves. If additional doses of fomepizole are required, the dose is increased to 15 mg/kg IV q12hrs for as long as necessary.10
In the management of acetaminophen toxicity, fomepizole is given as a one-time dose of 15 mg/kg IV.5 Fomepizole may be considered as an adjunctive therapy when concentrations of acetaminophen (µg/mL) and ALT (IU/L) drawn at the same time are multiplied together and yield a value of >10,000 µg/mL * IU/L, as these patients have a high likelihood of developing hepatotoxicity despite NAC administration.11
Adverse effects: The most common adverse effects attributed to fomepizole include headache, nausea, dizziness, somnolence, and metallic taste. Less common adverse effects include fever, bradycardia, transient transaminitis, rash, phlebitis, and eosinophilia.12 The safety and efficacy of fomepizole in pediatric patients has not been established.
Cost-effectiveness: Utilizing multimodal treatment strategies to acetaminophen overdose does not come without cost burden and should be thoroughly considered prior to initiation. The average cost of fomepizole for one dose is approximately $1,000.13 NAC approximately $5000 for oral routes and approximately $3000 for IV routes during a retrospective metanalysis in 2009.9 However, these costs pale in comparison to those of a liver transplant and its associated follow-up, estimated to cost up to $575,000.14
Conclusion
Acetaminophen toxicity is one of the most common causes of liver toxicity and reported poison center ingestions in the United States. NAC has been cited as the primary antidote for acetaminophen toxicity traditionally. However, based on new research, fomepizole may be used as an adjunctive treatment. The dual therapy has been suggested to be more efficient and hepatoprotective in patients at risk of developing acute liver failure secondary to massive acetaminophen overdose. The proposed dosing of fomepizole in these circumstances is 15 mg/kg IV once. By adding this single medication to the regimen, we can potentially protect unnecessary healthcare costs and save patients from risky and costly liver transplants.
Take-Home Points
- Acetaminophen overdose is a major cause of acute liver failure in the U.S.
- NAC is the primary antidote for acetaminophen toxicity
- Fomepizole may be used as an adjunctive treatment for patients at risk of developing acute liver failure due to acetaminophen overdose
- The dose of fomepizole used for acetaminophen toxicity is 15 mg/kg IV once
References
- Lee WM. Acetaminophen and the U.S. Acute Liver Failure Study Group: lowering the risks of hepatic failure. Hepatolog 2004;40(1):6-9.
- Suneil Agrawal, Babak Khazeaeni. Acetaminophen Toxicity. StatPearls, 2021.
- Larson AM, Polson J, Fontana RJ, et al. Acetaminophen-induced acute liver failure: results of a United States multicenter, prospective study. Journal of the American Association for the Study of Liver Diseases. 2005;42(6):1364-72.
- Woolum JA, Hays WB, Patel KH. Use of fomepizole, N-acetylcysteine, and hemodialysis for massive acetaminophen overdose. Am J Emerg Med.2020;38(3):692.e5-e7.
- Shah KR, Beuhler MC. Fomepizole as an adjunctive treatment in severe acetaminophen toxicity. Am J Emerg Med. 2020;38(2):410.e5-e6.
- Druteika DP, Zed PJ, Ensom MH. Role of fomepizole in the management of ethylene glycol toxicity. Pharmacotherapy. 2002;22(3):365-72.
- Akakpo JY, Ramachandra A, Jaeschke H. Novel strategies for the treatment of acetaminophen hepatotoxicity. Expert Opinion on Drug Metabolism and Toxicology. 2020;16(11):1039-50.
- Santiago R. Fomepizole: not just for toxic alcohol toxicity. CriticalCareNow, 25 Mar. 2021.
- Marchetti A, Rossiter R. Managing acute acetaminophen poisoning with oral versus intravenous N-acetylcysteine: a provider-perspective cost analysis. J Med Econ. 2009;12(4):384-91.
- Antizole (Fomepizole) information sheet. US Food and Drug Administration. 2020.
- Wong A, Sivilotti MLA, Dargan PI, et al. External validation of the paracetamol-aminotransferase multiplication product to predict hepatotoxicity from paracetamol overdose. Clinical Toxicology. 2015;53(8):807-14.
- Antizol (Fomepizole) injection [package insert]. Dover, DE: Paladin Labs: 2009.
- Prescription Price Comparison: Compare Drug Prices. WellRx.
- “How Much Does a Liver Transplant Cost?” CostHelper.