



Two techniques are currently utilized for guidewire insertion during central venous catheterization: introducer needle and angiocatheter over an introducer needle. But is one technique truly better than the other?
Introducer Needle
The vein is cannulated with the introducer needle, and the guidewire is directly passed through the hollow needle and into the vein. The disadvantage to this technique is that it requires the proceduralist to hold the needle steady as the guidewire is being introduced into the needle and subsequently the vein, resulting in the possibility of needle migration out of the vessel during guidewire insertion.
Angiocatheter Over an Introducer Needle
The vein is cannulated with the angiocatheter device, and the angiocatheter is threaded over the introducer needle into the vein. The needle is removed, and then the guidewire is inserted through the angiocatheter. The advantage to this technique is that it may provide more stable venous access during guidewire insertion and subsequently reduce the possibility of posterior wall puncture. The angiocatheter also facilitates using manometry to ensure the cannula is inside the vein and not the artery, particularly in situations where ultrasound cannot be utilized, such as subclavian central line placement.
Which Is Better?
Multiple studies have been performed to analyze this question in anesthesiology literature, but no studies have been performed in emergency medicine literature. Song et al. randomized pediatric patients undergoing surgery to either the use of an introducer needle alone versus the angiocatheter-over-introducer needle.1 In this study, both resident and attending anesthesiologists who had performed more than 50 central line insertions performed right or left internal jugular central venous catheterizations under ultrasound guidance. Ultimately the angiocatheter technique showed no superiority over using the introducer needle.
Two other studies by Lee et al. and Kim et al. used similar methods in adults. Lee et al. concluded that the rate of successful guidewire insertion on the first attempt was higher in the introducer needle group compared with the cannula. over-needle group (87.3% vs. 77.3%; p = 0.037).2 There were no significant differences in major complications. In the Kim et al. study, the introducer needle alone showed superiority.3 First-pass success rate was higher in the needle group compared with the catheter group (62.0% vs. 35.4% (p < 0.001), and the incidence of complications was significantly lower in the needle group compared with the catheter group (5.8% vs. 15.5%, respectively, p = 0.001).
While these 3 studies have concluded that the angiocatheter technique is not superior and may even be inferior to the introducer needle, there is still a role for using the angiocatheter. Arguably the angiocath may be most beneficial for early learners. In all 3 of the studies, the proceduralist was a skilled anesthesiologist who had performed 50+ lines, presumably using the traditionally taught Seldinger technique with the introducer needle alone. However, one of the most difficult steps in central line placement for beginners is keeping the introducer needle steady and threading the guidewire into the vein. The angiocath requires little skill to thread, and once the catheter is in, threading the guidewire is easy.
HOW TO PERFORM THE PROCEDURE
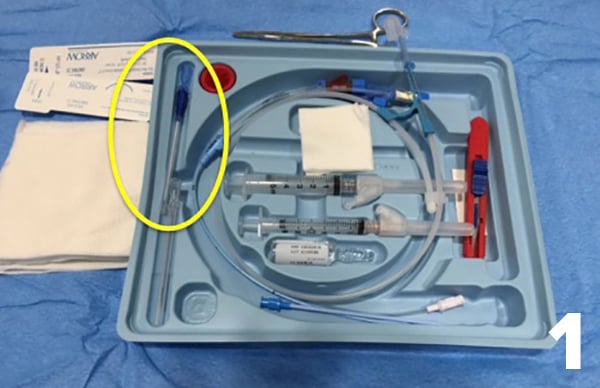
- Start the central line as usual. Wash your hands and don personal protective equipment. Prep the patient’s skin, create your sterile field, anesthetize the patient, and prep the central line kit. In the picture of the central line kit, the angiocath is circled in yellow.
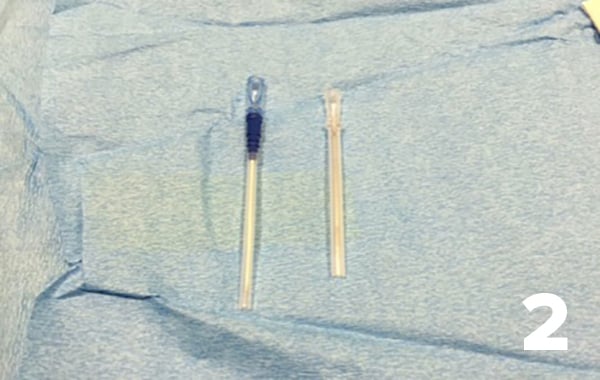
- Select the angiocatheter introducer needle, which is on the left in this picture. On the right is the regular introducer needle.
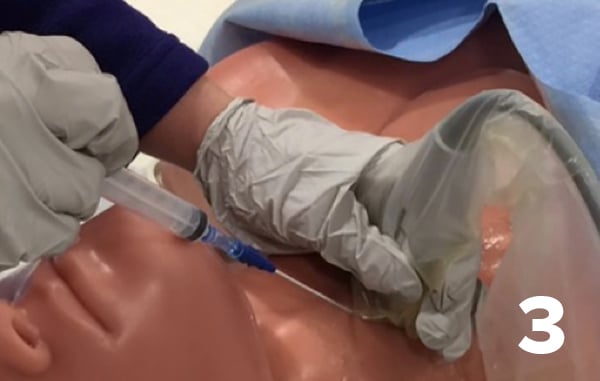
- Cannulate the vessel with the angiocatheter introducer needle, which can be confirmed by a flash of venous blood and on ultrasound. From personal experience, the angiocatheter introducer needle appears less echogenic on ultrasound than the regular introducer needle.
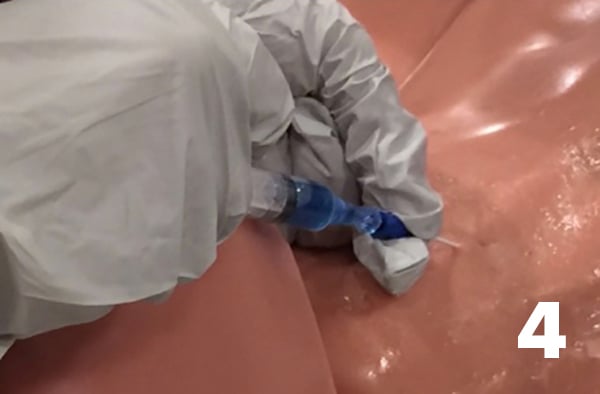
- Holding the introducer needle steady, thread the catheter over the needle, until the catheter hub is flush with the skin.
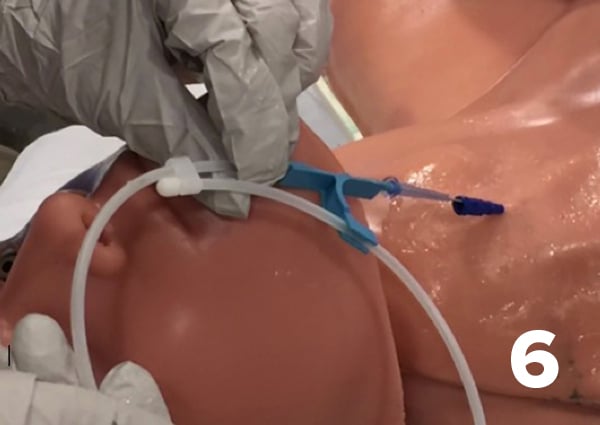
- Remove the introducer needle. Optional step: Now that you have stable venous access the angiocatheter can also facilitate venous confirmation with tubing used as a manometer.
- Insert the guidewire into the catheter. Thread the guidewire.
- Once the wire is threaded, remove the angiocatheter. 8 Continue the rest of the procedure as usual. Nick the skin with a scalpel, insert and remove the dilator, insert the multi-lumen catheter. Once the central line is in place, flush all ports, suture, and dress the line. Finally, confirm placement with chest x-ray.


References
1. Kim E, Kim BG, Lim YJ, et al. A prospective randomized trial comparing insertion success rate and incidence of catheterization-related complications for subclavian venous catheterization using a thin-walled introducer needle or a catheter-over-needle technique. Anaesthesia. 2016;71(9):1030-1036.
2. Lee YH, Kim TK, Jung YS, et al. Comparison of needle insertion and guidewire placement techniques during internal jugular vein catheterization: The thin-wall introducer needle technique versus the cannula-over-needle technique. Crit Care Med. 2015;43(10):2112-2116.
3. Song IK, Lee JH, Kang JE, et al. Comparison of central venous catheterization techniques in pediatric patients: needle versus angiocath. Paediatr Anaesth. 2015;25(11):1120-1126.