



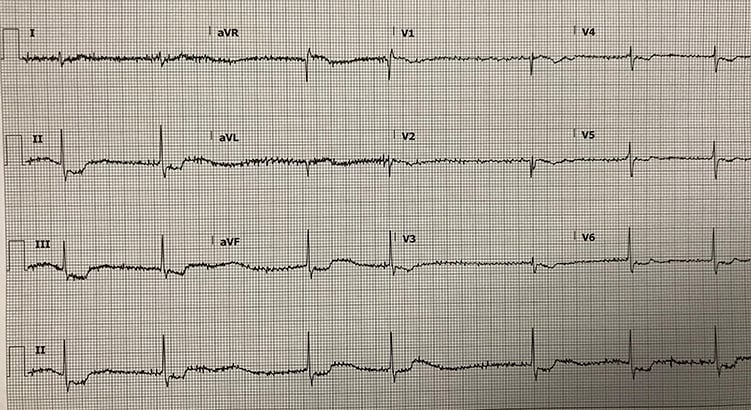
An 89-year-old female with atrial fibrillation presents with altered mental status. What is your interpretation of her ECG?
Digoxin Toxicity
This ECG shows atrial fibrillation with a slow ventricular response ~40 bpm and STD with TWI (also described as “scooped ST-segment/T-wave complexes”) in the inferior and mid-lateral precordial leads. The scooped ST-T complexes are best seen in leads with tall R-waves and are seen with therapeutic levels of digitalis derivatives (eg, digoxin). This what is commonly referred to as “digitalis effect,” or the Salvador Dali sign, and is not a sign of toxicity, only use. The presence of AFib with a slow ventricular response in the setting of digoxin use strongly suggests toxicity.
About Digoxin Toxicity
Digoxin, a cardiac glycoside, is a sodium-potassium ATPase blocker. Digoxin toxicity can be acute or chronic. Acute toxicity is typically caused by overdose of digitalis containing medications or ingestion of plants that contain cardiac glycosides such as foxglove, oleander, or Lily of the valley. Common causes of chronic toxicity include renal disease, electrolyte abnormalities, dehydration, and drug interactions. Chronic toxicity manifests over days to weeks and typically presents with vague symptoms that include anorexia, abdominal pain, nausea, and CNS symptoms. Hyperkalemia, more common in acute toxicity, is associated with a high mortality rate.
Dysrhythmias associated with digoxin toxicity are varied, and if digoxin toxicity were more common it would certainly compete with hyperkalemia for the title of the “syphilis of electrocardiography.” Common findings include PACs and PVCs, and dysrhythmias associated with toxicity include paroxysmal atrial tachycardia with variable block, accelerated junctional rhythms, AFib with slow ventricular response, and bidirectional VT.
First-line treatment for symptomatic dysrhythmias is digoxin immune FAB (eg, Digibind or DigiFab). Other treatments include atropine for bradycardias and AV blocks, and lidocaine or phenytoin for ventricular tachycardias if digoxin immune FAB isn’t available or effective.
Learning Points
Sodium-Potassium ATPase Blockers Toxicity
General Features
- Includes cardiac glycosides (eg, digoxin and digitalis derivatives)
EKG Features
- Seen with therapeutic levels
− Scooped ST-segment/T-wave complexes most pronounced in leads with tall R-wave (digoxin effect)
− PR lengthening
− QT shortening - Seen with toxicity
− Paroxysmal atrial tachycardia with variable block
− Accelerated junction rhythms
− Atrial fibrillation with slow ventricular response
− Bidirectional ventricular tachycardia (see Figure)
Clinical Significance
- Hyperkalemia is associated with a high mortality rate
- Treat with digoxin immune FAB when clinically indicated
Case Resolution
The patient’s labs showed worsening renal function and an elevated digoxin level twice the upper limit of therapeutic. Her heart rate normalized after treatment with digoxin immune FAB, and she was admitted to cardiology service.
For more information about ATPase blockers, please see p. 58 of the EMRA EKG Guide.