



A 62-year-old male presents with 1 hour of crushing chest pain radiating to the right shoulder.
What is your interpretation of the following ECG and what would you do next?
Answer
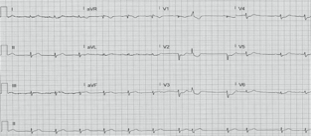
This EKG shows sinus rhythm at 72 bpm with a PVC (8th QRS complex followed by compensatory pause) and STD in I, aVL, and V2-V6. The STD in V2-V3 are concerning for a posterior MI, so a posterior EKG was obtained.
What is your interpretation of the following EKG and what would you do next?
Answer
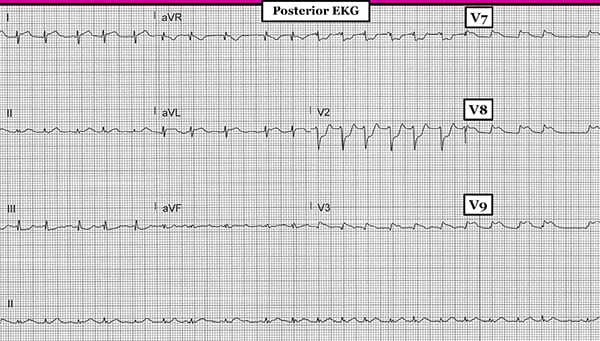
This EKG shows atrial fibrillation with a ventricular rate ~130 bpm, STE in aVL, V3, and V7-V9 with STD in III and V1-V2. The STE in V7-V9 meets AHA criteria for an acute posterior MI so the cath lab was activated.
Discussion
Isolated posterior, also called inferobasilar, MI is an important and easily missed diagnosis. Infarctions in this territory are typically seen with either an inferior or lateral MI, and in such cases portend a worse prognosis due to the larger area of ischemia. However, an estimated 3.3% of STEMIs are isolated posterior MIs and therefore do not show evidence of ST-elevation with standard lead placement.1
Diagnosing an isolated posterior MI requires using posterior leads (see Learning Points below). The criteria differ from traditional STEMI criteria in two important ways: there only needs to be 1 posterior lead with STE and the STE only needs to be ≥0.5 mm. The classic findings in leads V1-V3 on a standard ECG (i.e., no posterior leads) that are concerning for a posterior MI include deep horizontal STD, upright T-waves, and tall R-waves (which are equivalent to q-waves in an anterior MI, and are not present in our case above).
Posterior MI Learning Points
- Obtain a posterior EKG on any patient with a concerning story and isolated STD in V1-V3
- ≥0.5 mm STE in ≥ 1 posterior lead (V7, V8, or V9) diagnoses a posterior STEMI2
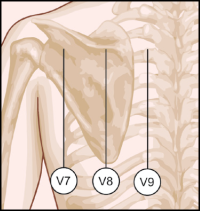
- Posterior lead placement (see image) is at the fifth intercostal space, parallel to the placement of V6, and moving lateral to medial:
- V7 - left posterior axillary line
- V8 - left mid-scapular line
- V9 - left paraspinal border3
Case Conclusion
The patient had a 100% occlusion of the distal RCA which was stented, and after a prolonged course in the cardiac ICU, the patient made a full recovery.
References
1. van Gorselen EOF, Verheugt FWA, Meursing BTJ, Oude Ophuis AJM. Posterior myocardial infarction: the dark side of the moon. Neth Heart J 2007;15(1):16-21.
2. Thygesen K, Alpert JS, Jaffe AS, et al. ESC/ACC/AHA/WHF Expert Consensus Document: Fourth Universal Definition of Myocardial Infarction (2018). Circulation. 2018;138(20):e618-e651.
3. Levis JT. ECG Diagnosis: Isolated posterior wall myocardial infarction. Perm J. 2015;19(4), e143-e144.