



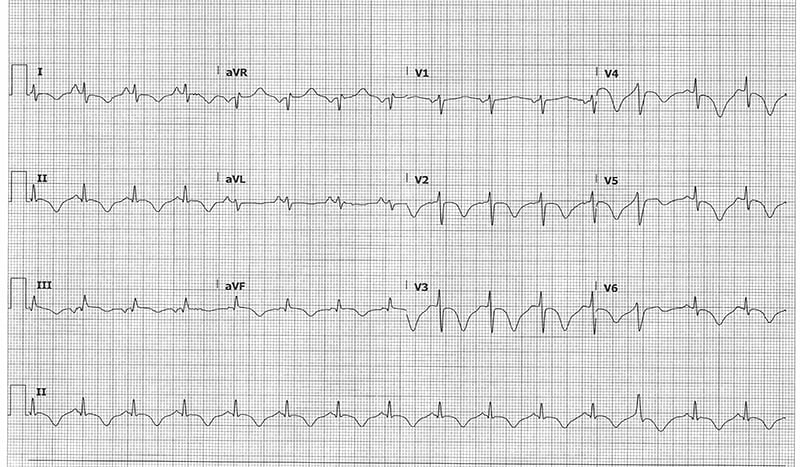
A 55-year-old female presents from home due to a brief episode of unresponsiveness and AMS. What is your interpretation of her ECG? (Bonus points if you identify the less obvious abnormality.)
Answer
This ECG shows normal sinus rhythm with a PVC (the 3rd to last beat) at a rate of 89 beats per minute, normal PR interval, normal QRS complex duration, prolonged QTc interval, and deep, wide, symmetric T-wave inversions in leads I, II, aVF and V2-V6. The less obvious abnormality is the presence of left arm-left leg (LA-LL) lead reversal.
Discussion
The T-wave represents ventricular repolarization. In the limb leads, the T-waves should always be upright in leads I and II, and inverted in lead aVR. The T-waves in leads III and aVL can be inverted or upright, and lead aVF will usually have an upright T-wave but may be flat or slightly inverted. In the precordial leads, the T-waves should always be upright in leads V5-V6 and usually upright in leads V1-V4. Inverted T-waves in lead V1 can be a normal variant, as are biphasic T-waves (upright then inverted) in the right precordial leads. In general, the T-wave amplitude is < 6 mm in the limb leads and < 10 mm in the precordial leads.
The differential diagnosis for inverted T-waves includes:
- Acute ischemia (early reciprocal changes)
- Bundle branch blocks
- Cardiomyopathies
- CNS injury
- Digitalis effect
- Intra-abdominal disorders
- Juvenile T-wave pattern
- LVH
- Metabolic abnormalities
- Pericarditis
- Pre-excitation syndromes
- Pulmonary embolism
- Toxicologic abnormalities
- Ventricular paced rhythms
- Wellens' type B
Given this patient's history, it would be reasonable to assume that these T-waves are cerebral T-waves.
This term is used to describe the broad, deep TWI seen with a variety of neurologic pathologies, including stroke, TIA, intracranial hemorrhage, and seizures. Cerebral T-waves are typically seen in the precordial leads and will often have an outward bulge in in the descending limb making them asymmetric. Other common ECG findings seen with CNS etiologies include QTc prolongation, seen in this ECG, and bradycardia.
Not many things cause such broad and deep TWI as seen in this ECG, so it is valuable to review the other possible causes, even if they don’t fit the clinical picture.
- Takotsubo cardiomyopathy can cause deep TWI and QTc prolongation. It can also present with STE that mimic a STEMI, and it can be difficult to differentiate the two clinically.
- Hypertrophic cardiomyopathy (HCM), more often the apical variant, can cause deep TWI with large R-waves in the precordial leads.
- Wellens' type B will show deep TWI, typically in leads V2-V3, suggestive of a critical stenosis/lesion of the proximal LAD.
- Pulmonary embolism can cause deep TWI in the inferior and right precordial leads.
This ECG shows LA-LL (left arm-left leg) lead reversal. A notable finding in this ECG that should prompt concern for LA-LL lead reversal is the prominent P-wave in lead I when compared to lead II. In general, the P-wave should be more prominent in lead II than lead I in normal sinus rhythm with correct lead placement.
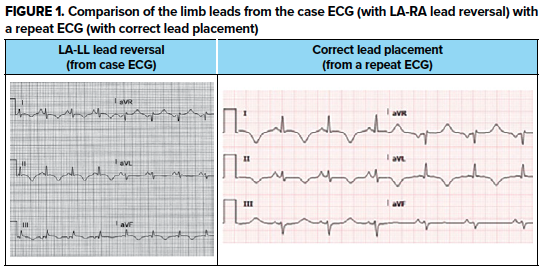
ECG findings seen with LA-LL lead reversal include (see Figure 1):
- Leads I and II "switch places," meaning that the normal findings in lead I are noted in lead II and vice versa
- Leads aVL and aVF "switch places," so the normal findings in lead aVL are noted in lead aVF and vice versa
- Lead III is inverted
- Lead aVR is unchanged
Case Conclusion
The patient underwent a broad workup, which was notable for a slightly elevated troponin and a normal head CT. A non-emergent cardiac catheterization showed clean coronaries and an echocardiogram showed apical hypokinesis diagnostic of Takotsubo cardiomyopathy. It was later discovered that the patient had been undergoing significant emotional stress at home, consistent with her diagnosis of Takotsubo. Note that this was a very atypical presentation for Takotsubo, which commonly presents with chest pain.
T-wave Learning Points
- Always upright in leads I, II, and V5-V6 and inverted in lead aVR
- TWI can be a normal variant in leads III, V1, and aVL (aVF may be slightly inverted)
- The differential diagnosis for TWI is broad and the workup should be based on clinical picture