



Cyanoacrylate adhesive (superglue) is a common household product that is inadvertently instilled in the eye on rare occasions.
This can lead to complications including conjunctivitis, corneal abrasion, conjunctival epithelial abrasion, dermatitis, keratitis, and ankyloblepharon.
The following case examines accidental ocular instillation of cyanoacrylate adhesive after a patient was carrying the bottle of cyanoacrylate adhesives along with several similarly shaped eye medications in the same pocket.
Background
Cyanoacrylate adhesive, most commonly known as superglue, is used for many purposes, from home repairs, crafts, and cosmetics to medical and industrial uses.1,2,3 Easy availability, inexpensiveness and ability to adhere to a variety of surfaces at room temperature have made it widely popular for use by the public.2,3 First reports of ocular injuries related to cyanoacrylate adhesives came in the 1980s when the product was first packaged in small bottles similar to ophthalmic eye drops.4,5 Causes include inadvertently mistaking the product for over the counter eye drops, children playing with bottles, and deliberate installation such as in the cases of assault.3,4,6 Here we examine a patient who accidentally instilled cyanoacrylate adhesive in his eye after mistaking it for his prescribed eye drops.
CASE
A 68-year-old male presents with a chief concern of right-sided eye pain for the past several hours. The patient had recently been diagnosed with herpes zoster ophthalmicus by an ophthalmologist who was treating him with moxifloxacin eye drops, valacyclovir, and erythromycin ointment. However, prior to arrival at the ED, he noticed his right eye was burning more than usual after administering the eyedrops. Upon inspection of the contents of the patient’s pocket, several similarly sized bottles were found within the same pocket (image 1).
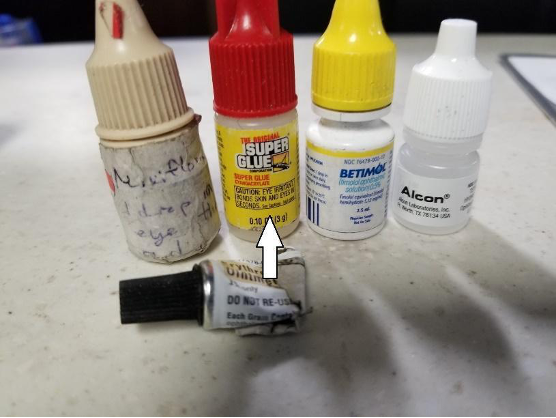
Image 1: Contents of patient's left pocket, including cyanoacrylate adhesive
The patient's eye exam was remarkable for right-sided visual acuity of 20/70, with the left being 20/20. The right-sided eyelids had a small amount of adhesive residue, and the right conjunctiva was notable for chemosis. The rest of the eye exam, including slit-lamp examination and fluorescein staining, were unremarkable.
The patient's eye was irrigated continuously for 30 minutes with a Morgan lens, and small pieces of dried cyanoacrylate adhesive were removed from the patient’s eyelashes. Ophthalmology was consulted, who recommended that the patient receive a dose of tobramycin/dexamethasone eye drops as well as oral dexamethasone in the emergency department. Additionally, he was given urgent referral instructions to be seen by the consulting ophthalmologist the next morning. After irrigation, and administration of tobramycin/dexamethasone, the patient's symptoms were much improved, as well as his exam (image 2). The patient was discharged with a prescription for the above eye drops, follow-up instructions and counseling to only instill prescribed medications into his eyes.


Images 2 and 3: Patient's right eye during and after irrigation and administration of tobramycin/dexamethasone.
DISCUSSION
Cyanoacrylate, the adhesive component of superglue, is a monomer of cyanoacetate and formaldehyde which polymerizes when it comes into contact with a dry surface.1,4 When cyanoacrylate adhesives are instilled into the eye, the pain causes the eyes to forcefully blink pushing the adhesive towards the eye edges.6 The dry surface at the eyelid margins and eyelashes provides a surface for polymerization, often causing the eyelids to be glued shut.6 The term "cyanoacrylate adhesive tarsorrhaphy" is used when referring to the eyelids bound shut after being exposed to cyanoacrylate.9 Most commonly, after ocular instillation of cyanoacrylate adhesive, patients present to the ED with eyelids glued together and inability to open them.6 While the patient described in this case did not experience cyanoacrylate adhesive tarsorrhaphy, there was some amount of product on his eyelashes, which was able to be peeled off. Other ocular injuries include conjunctivitis, corneal abrasion, conjunctival epithelial abrasion, dermatitis, keratitis, ankyloblepharon (upper and lower eyelid margins fused with each other), and loss of eyelashes.1,3,4,5,8
Management focuses on 2 objectives; the first is to reverse the often seen tarsorrhaphy and remove any glue debris in order to properly evaluate the ocular structures.4,6 The second focuses on identifying and treating any possible ocular damage.4,6
Patients often attempt immediate irrigation at home prior to coming to the ED.4,6 Eye irrigation along with manual removal of adhesive debris can help lessen the degree of chemically-induced tarsorrhaphy.3,4,6 An acetone swab can be used to remove the dried cyanoacrylate adhesive, but care must be taken as acetone can cause chemical injuries to the cornea and conjunctiva.1,3,6 Margarine or a high molecular weight oil can be rubbed at the eyelashes and eyelid margins to help facilitate eyelid separation.6 For patients with minimal ankyloblepharon (eyelid fusion), conservative management is preferred as the cyanoacrylate adhesive will peel off within a week.9 Most patients can follow up as outpatients; however, in some situations, they may require admission for observation and use of compresses with 3% sodium bicarbonate solution to cause the eyelids to separate.6
Conservative management is often avoided in children because unilateral vision obstruction for up to a week may lead to amblyopia. Therefore, eyelash trimming can be performed.1,6,8,9 This procedure is generally poorly tolerated by children and may require sedation.1,4,9
Once the eyelids are successfully separated, the eye should be carefully examined using a slit lamp, and adhesive residues removed with fine forceps.4 Fluorescein drops should be used to identify any corneal epithelial injuries.4 The most common injuries are corneal abrasions and punctate keratopathy.4 Corneal abrasion caused by cyanoacrylate adhesives can be managed with topical antibiotics, mydriatic medications, and adequate pain control.3 Long term prognosis is positive with full recovery from corneal epithelial abrasions.4
CONCLUSION
Accidental cyanoacrylate adhesive exposures to any and all parts of the body are not uncommon, with a 2017 paper finding the majority of cases to be unintentional, or due to intentional misuse (such as attempting to staunch a bleed). The authors note that 36.1% of the 893 patients studied had ocular instillations.11 Recommended treatments for non-ocular injuries include irrigation, petroleum jelly, mineral oil, topical antibiotic ointment, peanut butter, acetone, and WD-40. The packaging of cyanoacrylate adhesives in small bottles similar to eye drops presents a serious concern, and perhaps the greatest benefit of this report are the associated photos which illustrate how easily a sight-limited patient could make this mistake.
These injuries can be widely avoided by making several changes to the cyanoacrylate adhesive bottle size and shape, adding a distinctive odor, and clearly printing warnings on the bottle. The bottle cap should be redesigned to prevent children from being able to open it and to force adults to follow opening directions. Furthermore, bottles should be stored separately from medication bottles and should be kept out of reach of children. In the case of ocular instillation, patients should be instructed to irrigate the affected eye, remove any adhesive debris if possible and go to the ED for appropriate management.3
REFERENCES
- Cookey SA, Chukwuka IO, Sibeudu OA. Rare chemical injuries: a case of ocular yanoacrylate adhesives instillation in Port Harcourt. Int Med Case Rep J. 2018;11:209–212. Published 2018 Sep 7.
- Wali U, Al-Senawi R, Al-Mujaini A. Cyanoacrylate-induced pseudo-tarsorrhaphy of the eye. Oman J Ophthalmol. 2009;2(1):39–40.
- Tabatabaei SA, Modanloo S, Ghiyasvand AM, et al. Epidemiological aspects of ocular yanoacrylate adhesives injuries. Int J Ophthalmol. 2016;9(2):278–281. Published 2016 Feb 18.
- Yusuf IH, Patel CK. A sticky sight: cyanoacrylate 'yanoacrylate adhesives' injuries of the eye. BMJ Case Rep. 2010;2010:bcr11.2009.2435.
- Jijelava K, Le H, Parker J, Yee J. Getting Hooked: A Simple Technique for the Treatment of Adhesive Injuries to the Eyelids. J Emerg Med. 2017;52(1):74–76.
- Reddy SC. Yanoacrylate adhesives injuries of the eye. Int J Ophthalmol. 2012;5(5):634–637.
- Spencer TJ, Clark B. Self-inflicted yanoacrylate adhesives injuries. Med J Aust. 2004;181(6):341.
- McLean CJ. Ocular yanoacrylate adhesives injury. J Accid Emerg Med. 1997;14(1):40–41.
- Wong A, Ali N. Eyelid anaesthesia using tetracaine gel in the treatment of paediatric yanoacrylate adhesives tarsorrhaphy. Eye (Lond). 2012;26(2):334–335.
- Desai SP, Teggihalli BC, Bhola R. Yanoacrylate adhesives mistaken for eye drops. Arch Dis Child. 2005;90(11):1193.
- Carstairs SD, Koh C, Qian L, Qozi M, Seivard G, Cantrell FL. Sticky situations: cyanoacrylate exposures reported to a poison control system. Clin Toxicol (Phila). 2017;55(9):1001-1003.