



Case
A 5-week-old female born at term at 40 weeks via vaginal delivery presents for evaluation of a palpable mass in the right inguinal region. Mother states she initially noticed the mass one week prior to presentation and at times seemed to get bigger when the patient was crying or agitated. The patient initially presented to a local clinic and was referred to the emergency department for further evaluation. The mother reported that the patient had been eating appropriately every 4 hours, was producing an appropriate number of wet diapers and stools daily and was up to date on vaccinations. The physical exam showed a soft, non-tender and non-distended abdomen with normal bowel sounds; the patient had no vital sign abnormalities and was overall well-appearing. The inguinal mass had no fluctuance, overlying erythema or induration.
Bedside ultrasound was performed and demonstrated an oval-shaped, heterogeneous mass in the right inguinal region. The differential diagnosis included a bowel- or fat-containing hernia, hernia with ovarian content, enlarged lymph node, malignancy, or vascular malformation. The mass was located superficial to the abdominal musculature. The bladder and pubic bone were visualized. Further ultrasound examination revealed a hernia sac extending toward the labia, containing a heterogeneous mass with multiple embedded anechoic cystic structures. Color and pulse wave Doppler demonstrated internal vascular flow.

Image 1: Mass found on ultrasound
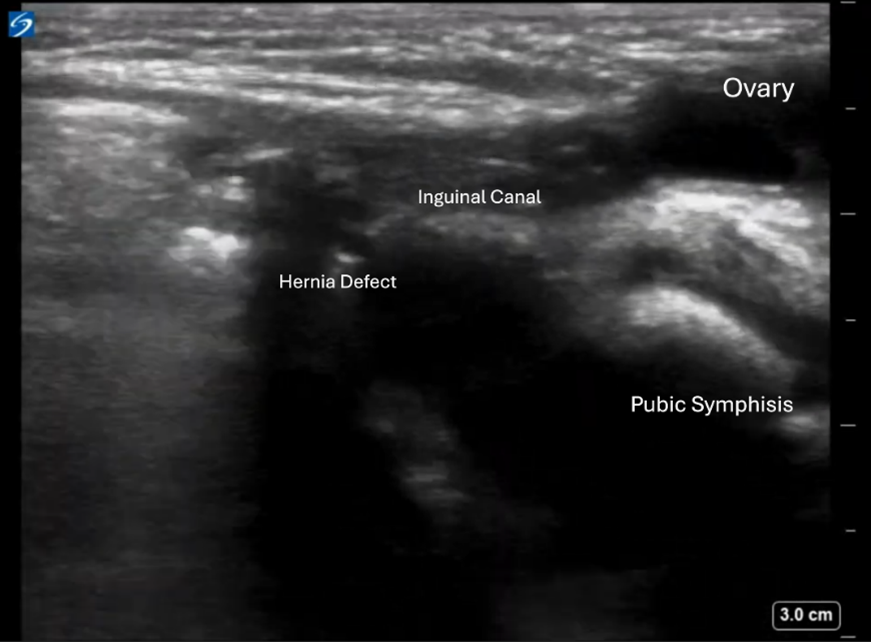
Image 2: Sagittal view. Hernia defect visualized with the hernia sac going towards the labia containing a heterogeneous mass, which appears to be an ovary.
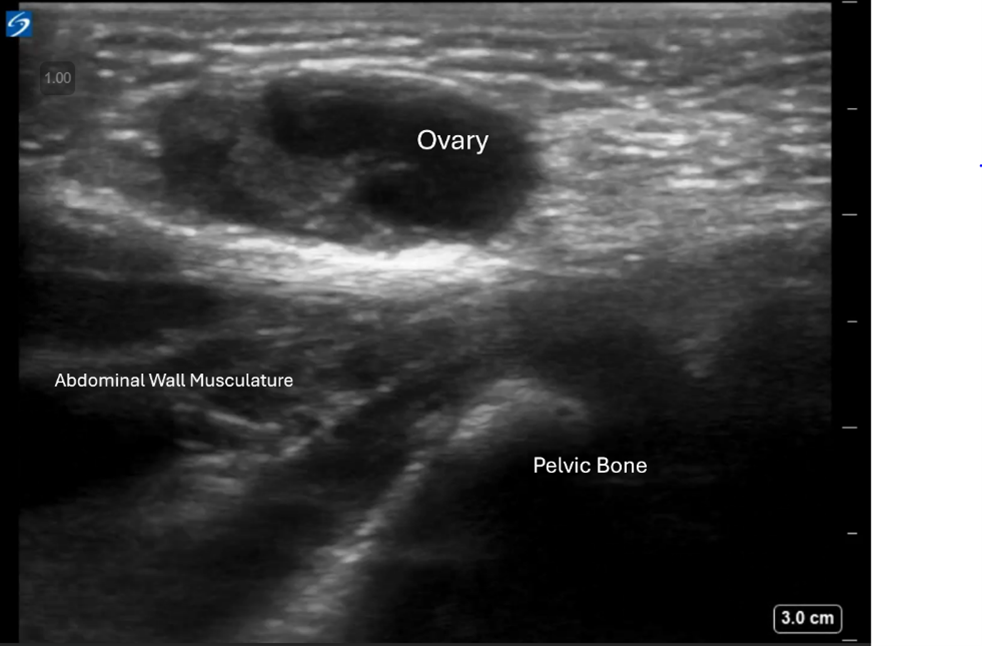
Image 3: Transverse view. The ovary is confirmed to be within the hernia sac and superficial to the abdominal wall musculature.
The contralateral (left) pelvis was scanned, showing a similar structure consistent with a normal-appearing ovary in its expected location. On returning to the affected side, the right ovary was absent from the pelvis. The inguinal mass was identified as the right ovary, herniated into the inguinal canal.
Inguinal hernias are a more common finding in males (who make up 90% of cases) compared to females (who make up 10% of cases). Inguinal hernias with ovarian tissue occur when an incomplete closure of the processus vaginalis allows the ovary (and possibly the fallopian tube) to descend into the inguinal canal. It is a rare condition typically seen in female infants and young girls, though it is not unheard of in women of reproductive age. Incidence of inguinal hernias with ovarian or fallopian tube content is 71% in children under 5 and approximately 30% in adolescents and women of reproductive age.3
Patients with inguinal hernias typically present with a painless groin swelling that changes in size with crying or straining. Diagnosis is usually made via trans-abdominal or pelvic ultrasound showing ovarian tissue in the hernia sac. Doppler blood flow is also performed to assess for ovarian torsion. Ultrasound findings include absence of one ovary in the lower pelvis and a groin mass with several small sonolucent cysts consistent with an ovary. The corpus luteum may or may not be present. Ultrasound can also be used to check the unaffected side for comparison. It is minimal risk and can expedite further workup. If the ultrasound findings are not definitive, computed tomography (CT) can also be used for confirmation. In the absence of concerning signs or symptoms, these hernias can often be treated non-emergently with surgical reduction of the hernia contents, ligation of the hernial sac, and closure of the deep inguinal ring. Non-absorbable mesh is also placed at the posterior wall of the inguinal canal to provide additional support.
Symptoms such as continued or worsening pain, tenderness, and persistent swelling or erythema are more concerning for incarceration and require emergent surgical management. In the case of ovarian involvement, these symptoms indicate possible torsion requiring prompt surgical detorsion to preserve ovarian function and reproductive capabilities. Although ovarian herniation into the inguinal canal is rare, approximately 4-11% of hernias with gynecologic structure involvement have an irreducible ovary; these are usually found intraoperatively. Of these cases, 2-33% have ovaries that are infarcted.2 This level of incidence highlights the importance of early diagnosis and treatment and explains why findings of ovarian involvement in the inguinal hernia are typically treated even if the patient is asymptomatic.
Given the patient’s findings on ultrasound, there was concern for an inguinal hernia with ovarian content and transfer was initiated to a pediatric hospital for further evaluation and management. At the pediatric hospital, the patient was evaluated and admitted to pediatric surgery, no CT imaging was performed, and the patient underwent open right inguinal hernia repair and diagnostic laparoscopy. Operative note confirmed that “a sliding hernia with tube and ovary in the hernia sac.” The ovary was described as pink and healthy. The hernia sac was placed into the abdominal cavity and the hernia defect was repaired. Per surgical report, the left side had no evidence of defect or hernia. The patient had an unremarkable post-operative course and was discharged the next day.
Key Points
- Inguinal hernias with ovarian contents are rare and are more common in the pediatric population than women of reproductive age.
- Inguinal hernias with ovarian content may appear on ultrasound as a small, round heterogenous mass with hypoechoic cystic structures. Bedside ultrasound can help with early diagnosis and management.
- Definitive treatment is almost always surgical management due to the high rates of irreducible and infarcted ovaries. A high index of suspicion must be maintained even in asymptomatic patients.
References
- Ariaya A, Yohannes B, Gebisa D, et al. When an inguinal hernia is more than just a hernia with ovary and fallopian tube involvement: a case report. J Med Case Reports 18, 436 (2024). https://doi.org/10.1186/s13256-024-04763-1
- Saini R, Bains L, Kaur T, et al. Ovarian inguinal hernia—a possibility in MURCS syndrome. J Ovarian Res 14, 114 (2021).
- Samantroy S, Mishra A, Panda J, et al. (December 31, 2021) Ovarian Inguinal Hernia in Premenopausal Women: A Case Report. Cureus 13(12): e20846.