



Although rare, chorea-hyperglycemia-basal ganglia syndrome is a presenting symptom of uncontrolled diabetes mellitus.
This condition is seen in elderly women, typically of Asian descent, with uncontrolled diabetes mellitus. Chorea-type movements have a broad differential diagnosis, including emergent and life-threatening conditions such as hemorrhage, infarction, malignancy, and infection. Less common causes of chorea movements include SLE, Huntington’s chorea, and Wilson’s disease. Patients classically present with hemichorea; however, bilateral chorea is also possible. The majority of patients have upper and lower extremities affected, with a smaller group having facial involvement. The treatment is decreasing the hyperglycemia and administering antipsychotics or benzodiazepines.
Case
A 61-year-old female with no previous past medical history presented to the emergency department with the chief complaint of involuntary movements. The patient reported 2 days of uncontrollable movements over the right side of her body. There was no associated numbness, focal weakness, visual changes, headaches, or speech difficulties.
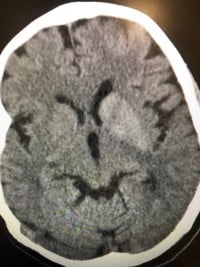
Physical examination revealed choreiform movements over the right upper and lower extremity. Neurological examination was otherwise benign without focal neurological deficit or sensation deficits. Vital signs were unremarkable. Laboratory workup was significant for a glucose of 396 without an anion gap metabolic acidosis and a sodium of 130. CT of the head showed hyperdensities in the basal ganglia bilaterally but greater on the left, compatible with calcifications.
The patient was admitted for further evaluation by neurology including an MRI, which showed chronic ischemic changes, most pronounced in the region of the left basal ganglia. Further laboratory workup showed an HbA1c of 14%. Neurology and endocrinology were consulted, who provided the patient with the diagnosis of chorea-hyperglycemia-basal ganglia syndrome (C-H-BG) caused by uncontrolled diabetes mellitus. The patient was started on insulin, valium, and was discharged in stable condition with neurology follow up.
Discussion
Chorea is defined as irregular, unpredictable, and brief jerky involuntary movements. Hemiballismus is defined as ballistic flinging movements. Both can be the result of central nervous system infections, neoplasm, intracranial hemorrhage, neurodegenerative disorders, drugs, toxins, and metabolic imbalances. The mechanism behind the cause of C-H-BG is unknown, although some theories have been postulated that include dopamine hypersensitivity or hyperactive dopaminergic states in postmenopausal women. Some debate that the cause is a direct effect of hyperglycemia on metabolism in the cerebrum, with hypoperfusion in the corpus in the striatum. Hyperglycemia is thought to cause favoring of anaerobic metabolism at a cellular level, which depletes gamma-aminobutyric acid (GABA) due to a substrate of GABA being quickly depleted in an anaerobic state. GABA functions to inhibit dopaminergic neurons in the nigrostriatal system and therefore a hyperglycemia-induced inhibition of GABA may lead to a hyperactive dopaminergic state, leading to the onset of chorea movements.
CT imaging shows hyperdensities in the striatal region of the caudate nuclei and putamen contralateral to the extremities affected by chorea. In cases of bilateral chorea movements, bilateral hyperdensities are seen. MRI classically shows high signal intensity of the basal ganglia lesion on T1 weighted MRI.
Treatment surrounds normalization of blood glucose. Patients can also be treated with antipsychotics such as clozapine, risperidone, and olanzapine or with medications with GABAergic properties such as benzodiazepines. In one study, a group of 16 patients were treated only with blood sugar control and had complete resolution of their chorea. In another case series, 74% of patients had complete resolution of their chorea within 10 months. A majority of patients reach full recovery within 6 months.
Case Resolution
The patient was discharged with outpatient follow-up. At follow-up with neurology, the patient’s choreiform movements had nearly resolved.
Take-Home Points
- Uncontrolled diabetes mellitus can present with abnormal choreiform movements.
- The differential diagnosis for choreiform movements includes Huntington’s disease, Sydenham chorea, Wilson’s disease, malignancy, SLE, hemorrhage, thyroid dysfunction, and drug-induced chorea.
- Patients affected by C-H-BG are predominantly elderly women with poorly controlled diabetes.
Resources
- https://www-uptodate-com.lecomlrc.lecom.edu/contents/overview-of-chorea?search=chorea&source=search_result&selectedTitle=1~115&usage_type=default&display_rank=1
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3989942/
- https://www.sciencedirect.com/science/article/pii/S0022510X19317150
- https://medicine.missouri.edu/sites/default/files/Hemichorea-manuscript-Final.pdf