



A middle-aged male presented to the ED for headache-like symptoms and was subsequently found to have a right temporal lobe mass upon magnetic resonance imaging.
Introduction
The temporal lobe is the most common site of origin of partial, also known as focal, seizures.1 Partial seizures are the most common seizure type in adults and usually occur in the mesial, or middle, temporal lobe. The most common cause of temporal lobe epilepsy (TLE) in middle-aged adults is hippocampal or mesial temporal sclerosis secondary to neuron cell death, accounting for over 80% of TLE cases.1 Other less frequent causes include tumors, infection, perinatal injuries, vascular malformations, encephalitis, and genetic mutations.1 TLE can be further broken down into two types. Simple partial, or focal aware, seizures occur without impairment of consciousness and can be subdivided into motor and non-motor (somatosensory, autonomic, and/or psychological) seizures.2 Complex partial, or focal impaired, seizures involve some degree of altered consciousness and are often preceded by a simple partial seizure, typically an aura that lasts anywhere from seconds to minutes before the impairment of consciousness occurs.3
Case
A 40-year-old male with a past medical history of migraines, anxiety, depression, and hyperlipidemia presented to the ED for evaluation of a sensation in his head that he described as pressure and fullness. He further elaborated that this sensation was “not a headache” and unlike his past migraines. He had experienced similar episodes in the past, though they occurred 1-2 times a month for years and lasted for 15-20 minutes. However, this episode began the day prior to arrival while at work as a schoolteacher and lasted several hours.
This episode was associated with difficulty breathing, nausea, chills, diaphoresis, feelings of anxiety, hypersomnolence, difficulty walking straight (which the patient described as though he was “drunk” when walking), and altered sensation of smell (which he describes as “abnormal smells”).
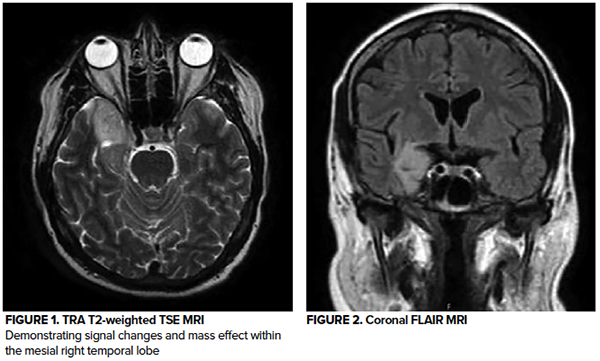
An MRI of the brain demonstrated an area of signal changes consistent with a mass effect in the mesial right temporal lobe. Neurology evaluated the patient and started him on levetiracetam 750 mg every 12 hrs. He was admitted to the hospital for further evaluation and symptom control.
Discussion
The complexity and variety of signs and symptoms associated with temporal lobe epilepsy make this condition notably difficult to diagnose.4 This patient demonstrated features that walk the line of simple versus complex partial.
He had an aura (unpleasant smells) and likely postictal state (hypersomnolence, "feeling drunk" while walking), which are both typical of complex partial seizures.3, *** However, he did not experience any loss of consciousness, which is a defining component of complex partial seizures.6 He also did not report typical automatisms (such as chewing and lip-smacking)that often precede and are predominant in complex partial seizures, occurring in about 40-80% of patients with temporal lobe epilepsy.3
Our patient also demonstrated autonomic and somatosensory alterations that are common in simple partial seizures.2 This was evidenced by olfactory hallucinations and a multitude of autonomic dysfunctions, including nausea, diaphoresis, and chills. Though difficult to tease out in our patient secondary to his underlying history of anxiety and depressions, psychological features are a common presentation of non-motor simple partial seizures.2 Interestingly, complex partial seizures have also been found to be first misdiagnosed as a primary psychiatric illness.7 Therefore both simple and complex partial seizures should be kept on the differential diagnosis of acute and transient psychotic behavior, particularly irrational and aggressive behavior.4
Overall, this patient demonstrated symptoms of both simple and complex partial seizures. HIs multitude of symptoms highlights the complexity and often difficult diagnosis of temporal lobe epilepsy. Of note, a direct cause, such as a mass effect, is not found in up to 25% of TLE cases, which can further delay diagnosis.8
Case Conclusion
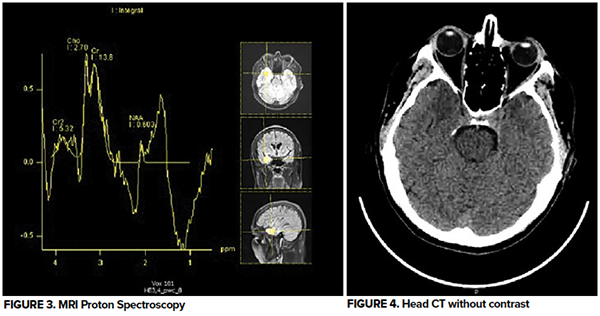
During admission, the patient was continued on his regimen of levetiracetam 750 mg two times daily and did not experience any further episodes overnight. He was discharged the following day and followed up with neurology and neurosurgery for MR spectroscopy and further management. Post-admission, he experienced some seizure activity and was switched to oxcarbazepine, which he tolerated well aside from experiencing some fatigue. The pathology of his tumor showed a “multinodular vacuolating neuronal tumor” and he subsequently underwent a full surgical resection of the tumor, and has been doing well at the time of this publication.
References
- Blair RDG. Temporal lobe epilepsy semiology. Epilepsy research and treatment vol. 2012 (2012): 751510. doi:10.1155/2012/751510
- Kumar A, Maini K, Arya K, et al. Simple Partial Seizure. [Updated 2021 Jul 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK500005/
- Kumar A, Sharma S. Complex Partial Seizure. [Updated 2021 Jun 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519030/
- Walter RD. Clinical aspects of temporal lobe epilepsy--a review. California medicine vol. 110,4 (1969): 325-9.
- Abood W, Bandyopadhyay S. Postictal Seizure State. [Updated 2021 Jul 16]. In: StatPearls [Internet]. Treasure Island (FL).: StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526004/
- Englot DJ, Blumenfeld H. Consciousness and epilepsy: why are complex-partial seizures complex?. Progress in brain research vol. 177 (2009): 147-70. doi:10.1016/S0079-6123(09)17711-7
- Sultan S, Fallata EO. A Case of Complex Partial Seizures Presenting as Acute and Transient Psychotic Disorder. Case reports in psychiatry vol. 2019 1901254. 2 May. 2019.
- Cleveland Clinic. Temporal Lobe Epilepsy: Causes, Symptoms, Diagnosis & Treatment. Available at: https://my.clevelandclinic.org/health/diseases/17778-temporal-lobe-seizures.