



Ch. 3 - Chest Pain
David Mai, MD, MPH | Crozer-Chester Medical Center
Richard Pescatore, DO, FAAEM | Delaware Division of Public Health
Approximately 8 million patients visit the emergency department (ED) each year for chest pain in the United States, for an estimated health care cost of $5 billion.1 Chest pain is a complicated presentation, with analgesic management focusing on the underlying cause.
Physicians not only need to rule out acute life-threatening causes of chest pain but must also provide patients with safe and timely pain relief. For patients with non- life-threatening causes of chest pain—including but not limited to costochondritis, pericarditis, rib and sternum fractures—a pharmacological regimen that is quick and effective will allow physicians to promptly and safely treat patients and ensure the best possible outcome. The purpose of this chapter is to discuss the safe and efficacious pain management options for common non-life-threatening causes of chest pain.
Differential Diagnosis of Chest Pain (non-life-threatening)
Due to the vast number of conditions that cause chest pain, the first step in managing chest pain is to consider and eliminate the life-threatening causes. For all patients presenting chest pain, it is vital to initially evaluate for and exclude cardiac and pulmonary contusions, cardiac tamponade, aortic dissection, acute coronary syndrome, cardiac tamponade, pulmonary embolism, spontaneous/tension pneumothorax, and Boerhaave syndrome/esophageal rupture. The focus of this chapter will be on the three most common sources of non-life-threatening chest pain encountered in the emergency setting: costochondritis, rib/sternal fractures, and pericarditis.
(Note – the management of life-threatening causes of chest pain is dependent on a number of factors including hemodynamic stability and ongoing resuscitation efforts, which must be managed on a case-by-case basis; as such, a discussion of pain management in the setting of life-threatening pathology is beyond the scope of this chapter.)
Costochondritis
Diagnosis. Costochondritis (CC) is a common musculoskeletal cause of chest pain triggered by inflammation of the costal cartilages. CC is a clinical diagnosis notable for chest pain that is commonly reproducible by palpation or with the movement of the upper extremities. The presence of at least two of the following four symptoms is associated with a diagnosis of costochondritis: localized muscle tension, stinging pain, pain reproducible by palpation, and the absence of cough.2 The "crowing rooster" maneuver can also aid in the diagnosis of costochondritis. The "crowing rooster" maneuver involves the patient looking toward the ceiling to extend their neck while dorsally extending their arms while the provider - standing behind the patient - exerts dorsal traction on the extended arms, which reproduces the chest pain in costochondritis.3
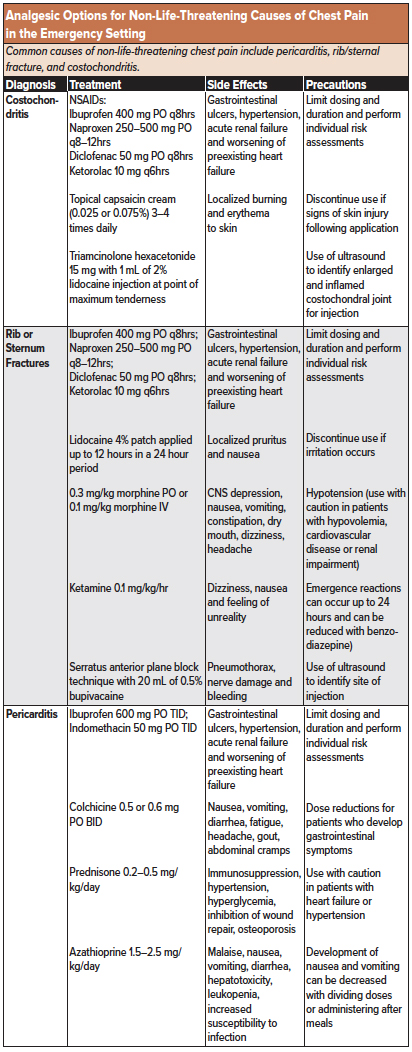
Treatment. In general, the use of opioids should be avoided for (atraumatic) musculoskeletal pain. Initial analgesic management for costochondritis involves a short course of either oral or parenteral analgesic medications. For mild pain, low to moderate doses of acetaminophen (650-975 mg PO) or a nonsteroidal anti-inflammatory drug (NSAID) such as ibuprofen, diclofenac or naproxen should be considered first-line. Patients may respond differently to various subclasses of NSAIDs,4 but data is currently lacking. Topical analgesic agents such as capsaicin cream (applied 3-4 times daily 5) or topical NSAIDs (diclofenac, ibuprofen, ketoprofen, and piroxicam) may be considered as a form of localized analgesic distribution to limit total-body quantities of NSAIDs delivered. Alternatively, a mixture of 15 mg of triamcinolone hexacetonide (glucocorticoid corticosteroid) and 1 mL of 2% lidocaine can be safely injected at the point of maximum tenderness by identifying the enlarged and inflamed costochondral joint using ultrasound guidance.6 Any activity that worsens the chest pain, including (but not limited to) lifting or pushing heavy objects should be minimized during the recovery period.3
Rib and Sternum Fractures
Diagnosis. Patients with blunt thoracic trauma may develop moderate to severe chest pain secondary to rib or sternum fractures. While chest radiographs are typically used to screen patients with blunt thoracic trauma, up to 50% of rib fractures go undetected.7 Among patients with suboptimal radiographic imaging due to pain-induced abnormal respiratory effort or reduced air-entry, a computerized tomography (CT) scan of the thorax can improve the sensitivity of diagnosing rib or sternum fractures.8 Although a minimal difference in outcome has been shown between patients with rib fractures identified by CT alone (ie, missed on plain radiograph),9 the number of fractured ribs is directly related to the reduced tidal volume and coughing effort10 and the probability of developing an associated pulmonary infection,11 underscoring the importance of adequate analgesia.
Treatment. Patients with mild to moderate pain who can tolerate oral medications should be initiated on oral acetaminophen and either oral NSAIDs (ibuprofen, diclofenac or naproxen) or IV NSAIDs (15 mg ketorolac IV) for maintenance analgesia with low-dose opioids (eg, 0.1–0.3 mg/kg morphine PO or 0.05–0.1 mg/kg morphine IV) used for breakthrough pain. Application of topical lidocaine patches has been shown to significantly lower rib fracture-associated pain.12 Ketamine may also be considered a safe and effective analgesic alternative to opioids. A single dose of sub-dissociative ketamine (0.1–0.2 mg/kg IV) or a continuous intravenous infusion (0.1 mg/kg/hr) may be used as a complement to acetaminophen and NSAIDs.13 For pain refractory to the analgesic agents described above, regional anesthesia can and may also be performed (ultrasound-guided serratus anterior plane block, intercostal nerve block, or erector spinae block). For a serratus anterior plane block, the lateral cutaneous branches of the thoracic intercostal nerves (T2–T12) localized to the plane superficial to the serratus anterior muscle are anesthetized with 15-20 cc of 0.5% bupivacaine for long-term pain reduction.14 This plane is best visualized in the mid-axillary line at the level of the nipple.15 For isolated rib fractures, an intercostal nerve block may also be considered using 5-10 cc 0.5% bupivacaine as an alternative with fewer risks of adverse effects. However, it should only be performed by experienced providers under ultrasound guidance due to an increased risk of pneumothorax.16 (See the nerve block chapter for an in-depth discussion of safely and effectively performing nerve blocks in the emergency setting). For severe pain refractory to the previously mentioned analgesic alternatives, patient-controlled analgesia (PCA) pumps may be considered with opioids such as morphine.
Pericarditis
Diagnosis. Pericarditis refers to the inflammation of the pericardial sac caused by a number of disease processes, including infection, malignancy, uremia, radiation, connective tissue disease (rheumatoid arthritis, systemic lupus erythematosus, ankylosing spondylitis, or cardiac injury). However, the underlying etiology of pericarditis in most patients is never identified. Patients are classically presenting with sharp, pleuritic chest pain and a friction rub on the exam. In addition, an electrocardiogram may classically show widespread ST elevations or PR depressions. A pericardial effusion may also be identified under ultrasound guidance. Inflammatory markers (ESR, CRP) may assist in confirming the diagnosis, though not the underlying etiology.
Treatment. The goals of treating pericarditis include pain relief, resolution of inflammation, and prevention of recurrence. Initial treatment includes oral NSAIDs (diclofenac, acetaminophen, naproxen) and colchicine as well as a reduction in strenuous activity during the recovery period. For patients with contraindications to NSAIDs, glucocorticoids may be used, though they are associated with a higher risk of pericarditis recurrence.18 According to expert opinions, patients suffering from pericarditis should not participate in competitive sports for three months.19,20
Disposition from the ED
While the ultimate goal of chest pain management is to improve the quality of life by returning the patient to their baseline functional status, elimination of pain may not be feasible. Instead, the goals should be enough of a reduction to allow the patient to continue their daily activities during a painful condition.21
Educate the patient regarding their chest pain pathology and provide anticipatory guidance for improvement and potential complications such as fever, worsening cough or shortness of breath, persistent chest pain, or any other concerning symptoms. Discharge with an incentive spirometer to maintain pulmonary function.
Analgesic prescriptions should function only as a bridge to a primary care provider or pain clinic follow up, and a combination of oral acetaminophen or ibuprofen are considered to be first-line. If opioids are required for outpatient management, prescriptions should be limited to 2 to 3 days of short-acting alternatives 20. If the patient is unable to successfully fill their prescription prior to the return of their pain, consider discharging them with a 'starter pack' of ibuprofen/acetaminophen to ensure analgesic availability. Establishing outpatient follow-up with a primary care provider or pain management specialist provides care continuity and limits the risk of oligoanalgesia as an outpatient. Dysphoria and an increased adverse side effect profile, when taken at supratherapeutic doses, make oral morphine sulfate immediate-release (MSIR) a preferred analgesic when a short opioid prescription is required.21,22 [Recommended guideline: 3-day supply of MSIR 15 mg q4-6 hours with a plan for re-evaluation if pain persists beyond 3 days.]
Summary
The treatment of chest pain can be a complicated task in the emergency department, as there are many life-threatening and non-life-threatening causes. The initial evaluation should always include the necessary diagnostic tests and imaging modalities needed to exclude the life-threatening causes. Depending on the underlying source of pain, symptomatic relief may be accomplished through a combination of both oral and parenteral analgesia. In treating the pain, it is essential to inform patients that their symptoms will likely not be fully resolved during their stay in the emergency department and that continued analgesic management with oral analgesics will often be needed in the outpatient setting. As with all pain pathologies treated in the emergency setting, it is important to provide return precautions for worsening or new symptoms such as shortness of breath, dizziness, nausea, vomiting, persistent fevers or worsening chest pain that may indicate an alternative source of pain and a need for prompt re-evaluation.
References
- Paichadze N, Afzal B, Zia N, Mujeeb R, Khan M, Razzak JA. Characteristics of chest pain and its acute management in a low-middle income country: analysis of emergency department surveillance data from Pakistan. BMC Emerg Med. 2015;15 Suppl 2:S13.
- Bosner S, Becker A, Hani MA, et al. Chest wall syndrome in primary care patients with chest pain: presentation, associated features, and diagnosis. Fam Pract. 2010;27(4):363-369.
- Ayloo A, Cvengros T, Marella S. Evaluation and treatment of musculoskeletal chest pain. Prim Care. 2013;40(4):863-887, viii.
- Pescatore R. When Ibuprofen Fails, Naproxen Isn't the Answer. Emergency Medicine News. 2018;40(4):10. Accessed 10/10/2019.
- Rains C, Bryson HM. Topical capsaicin. A review of its pharmacological properties and therapeutic potential in post-herpetic neuralgia, diabetic neuropathy and osteoarthritis. Drugs Aging. 1995;7(4):317-328.
- Kamel M, Kotob H. Ultrasonographic assessment of local steroid injection in Tietze's syndrome. Br J Rheumatol. 1997;36(5):547-550.
- Bansidhar BJ, Lagares-Garcia JA, Miller SL. Clinical rib fractures: are follow-up chest X-rays a waste of resources? Am Surg. 2002;68(5):449-453.
- Traub M, Stevenson M, McEvoy S, et al. The use of chest computed tomography versus chest X-ray in patients with major blunt trauma. Injury. 2007;38(1):43-47.
- Murphy CEt, Raja AS, Baumann BM, et al. Rib Fracture Diagnosis in the Panscan Era. Ann Emerg Med. 2017;70(6):904-909.
- de Campos JRM, White TW. Chest wall stabilization in trauma patients: why, when, and how? J Thorac Dis. 2018;10(Suppl 8):S951-S962.
- Ho SW, Teng YH, Yang SF, et al. Risk of pneumonia in patients with isolated minor rib fractures: a nationwide cohort study. BMJ Open. 2017;7(1):e013029.
- Zink KA, Mayberry JC, Peck EG, Schreiber MA. Lidocaine patches reduce pain in trauma patients with rib fractures. Am Surg. 2011;77(4):438-442.
- Walters MK, Farhat J, Bischoff J, Foss M, Evans C. Ketamine as an Analgesic Adjuvant in Adult Trauma Intensive Care Unit Patients With Rib Fracture. Ann Pharmacother. 2018;52(9):849-854.
- Wurnig PN, Lackner H, Teiner C, et al. Is intercostal block for pain management in thoracic surgery more successful than epidural anaesthesia? Eur J Cardiothorac Surg. 2002;21(6):1115-1119.
- Nagdev A MD, Durant E, Herring A. The ultrasound-guided serratus anterior plane block. ACEP Now. 2017;36(3):12-13.
- Hwang EG, Lee Y. Effectiveness of intercostal nerve block for management of pain in rib fracture patients. J Exerc Rehabil. 2014;10(4):241-244.
- Dean M. Opioids in renal failure and dialysis patients. J Pain Symptom Manage. 2004;28(5):497-504.
- Farand P, Bonenfant F, Belley-Cote EP, Tzouannis N. Acute and recurring pericarditis: More colchicine, less corticosteroids. World J Cardiol. 2010;2(12):403-407.
- Daskalov IR, Valova-Ilieva T. Management of acute pericarditis: treatment and follow-up. European Society of Cardiology. 2017;15. Accessed 10/01/2019.
- Dauphin C, Merlin E, Chalard A, Trésorier R, Soubrier M. Recurrent pericarditis: current challenges and future prospects. Research Reports in Clinical Cardiology. 2016:99–108.
- Lee TH. Zero Pain Is Not the Goal. JAMA. 2016;315(15):1575-1577.
